Double Board Certified · Functional Nasal Surgery
Nasal Valve Collapse Treatment in NYC — structural support for the breathing nose.
Nasal valve collapse treatment in NYC with Dr. Moustafa Mourad. Compare spreader, alar rim, batten, and lateral crural strut grafts for blocked breathing.
ABFPRS
Facial Plastic & Reconstructive Surgery
ABOto
Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
In Consultation
"Patients have often been told for years that there is nothing wrong, when the nasal valve has been quietly collapsing on every breath."
A Note from Dr. Mourad
"Nasal valve collapse is one of the most under-diagnosed structural causes of nasal obstruction. When it is the right diagnosis, structural reconstruction — cartilage grafting that supports the sidewall — produces durable improvement."
— Dr. Moustafa Mourad, MD
Medically reviewed by Moustafa Mourad, MD, FACS — dual board-certified Facial Plastic & Reconstructive Surgeon and Otolaryngologist (Head & Neck Surgery).
Last reviewed: June 2026
Is this the right page for you?
This page is for
- You feel your nose collapse or pinch closed when you breathe in deeply.
- Breathing strips help, which often points to a weak or narrow nasal valve.
- Previous surgery, injury, or naturally weak cartilage has left the sidewall unsupported.
You may be looking for
- If the blockage is from a deviated septum, see septoplasty.
- If enlarged turbinates are the cause, see turbinate reduction.
Key takeaways
- Nasal valve collapse narrows the airway's tightest point, so breathing worsens when you inhale deeply.
- Cartilage grafts reinforce the weak sidewall — the structural fix that holds the airway open over time.
- Diagnosis is made on examination, including the Cottle maneuver, not on imaging alone.
- Spreader grafts support the internal valve and middle vault; rim, batten, and lateral crural strut grafts provide site-specific support of the external valve and sidewall.
- Repair can be purely functional, or combined with rhinoplasty when shape is also a concern.
Overview
What is nasal valve collapse treatment?
Nasal valve collapse treatment is a structural surgical procedure that reinforces the internal and/or external nasal valves — the narrowest segments of the nasal airway — using cartilage grafts harvested from the septum, ear, or rib. Common techniques include spreader grafts, alar batten grafts, and lateral crural strut grafts.
It is considered when a patient has persistent nasal obstruction that worsens with deep inspiration or exercise, when the sidewalls of the nose visibly collapse on breathing in, and when manual lateralization (Cottle maneuver) improves airflow. The diagnosis is made on examination, not on imaging alone.
When the cosmetic shape of the nose is also a concern, valve reconstruction can be combined with rhinoplasty so both function and form are addressed in one operation. When the only concern is breathing, the operation is purely functional and the external shape is preserved.
What is nasal valve collapse?
The nasal valve is the narrowest part of the airway. When its cartilage support is weak, the sidewall of the nose can draw inward as you breathe in, restricting airflow even when the septum is straight.
Because the problem is structural, treatment focuses on restoring support to the sidewall rather than removing tissue — which is why a straightened septum alone does not always resolve the obstruction.
How do I know if I have nasal valve collapse?
Common signs include a sidewall that visibly draws inward on inhalation, breathing that improves when you gently pull the cheek outward (the Cottle maneuver), and obstruction that persists after septum-focused treatment. A definitive diagnosis requires an examination of the valve area at rest and during breathing.
Self-tests can suggest the diagnosis, but they cannot distinguish internal from external valve collapse or rule out other causes of obstruction — that assessment is made at consultation.
Can septoplasty fix nasal valve collapse?
Not by itself. Septoplasty straightens the septum, but valve collapse is a weakness of the sidewall cartilage — a separate structural problem. When both are present, they are often addressed together in one operation.
This distinction is one of the most common reasons breathing remains blocked after a technically successful septoplasty.
Septoplasty in NYCWhat is the difference between internal and external nasal valve collapse?
The internal valve is the narrow angle between the septum and the upper lateral cartilage, midway up the nose; the external valve is the nostril rim and its supporting cartilage. Internal collapse typically causes obstruction deeper in the nose, while external collapse shows as a nostril that pinches inward on inhalation.
The two are repaired differently — spreader grafts commonly support the internal valve, while rim or batten grafts support the external valve — so identifying which valve is involved shapes the surgical plan.
Meet Dr. Mourad
A nasal valve repair surgeon who understands why a straight septum may still not breathe.
Dr. Moustafa Mourad treats nasal valve collapse as a structural airway problem that is often missed when evaluation stops at the septum. Many patients have already tried sprays, strips, or even septoplasty and still feel that one side of the nose closes when they inhale, exercise, or sleep. The reason may be weakness or narrowing of the internal or external nasal valve rather than inflammation alone.
Dr. Mourad is dual board-certified in Facial Plastic and Reconstructive Surgery and Otolaryngology–Head and Neck Surgery. In nasal valve consultations, he evaluates dynamic sidewall collapse, static narrowing, the internal valve angle, lower lateral cartilage strength, septal deviation, turbinate size, prior rhinoplasty, prior trauma, and the patient’s response to maneuvers such as the Cottle or modified Cottle test.
His philosophy is that nasal valve repair must be tailored to the exact area of weakness. Some patients need spreader grafts for internal valve narrowing; others need alar batten grafts, lateral crural strut grafts, or revision functional rhinoplasty to restore lower sidewall support. Minimally invasive options such as radiofrequency remodeling or absorbable implants may help selected patients, but they are not substitutes for structural reconstruction when cartilage has been over-resected, scarred, or weakened. The goal is a stable airway that improves breathing without creating an unnatural nasal shape.
- Dual board-certified facial plastic surgeon and otolaryngologist
- Evaluates internal and external nasal valve collapse, septum, turbinates, and prior surgery together
- Structural approach to spreader grafts, batten grafts, lateral crural support, and revision functional rhinoplasty
- Practice focused on nasal airway, reconstructive, sinus, and facial surgery
An Established Academic Authority
Double board certification. Fellowship director. Published author. A surgeon's surgeon.
ABFPRS
Board Certified
American Board of Facial Plastic & Reconstructive Surgery
ABOto
Board Certified
American Board of Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
American Academy of Facial Plastic and Reconstructive Surgery
Textbook
Published Author
Contributions to the academic literature of facial plastic surgery
Dual board certification in both Facial Plastic & Reconstructive Surgery and Otolaryngology — Head & Neck Surgery.
01 · Why Dr. Mourad
Diagnosis first, then a plan that fits.
Dr. Mourad evaluates the nasal valve specifically at every functional consultation — collapse is missed when it is not actively looked for.
When valve collapse is the diagnosis, structural grafting with autologous cartilage is the durable answer; non-structural in-office options are discussed candidly.
Function is the goal; cosmetic change is a side effect that is planned, not stumbled into.
02 · Ideal Candidates
Who benefits most from this operation.
Candidacy is determined together at consultation. The most satisfied patients share three things in common.
I
Inspiratory Collapse
Patients whose nostrils visibly collapse inward with strong inhalation, or whose breathing improves with the Cottle maneuver (lateral pull on the cheek).
II
Failed Septoplasty
Patients who have had septoplasty without breathing improvement — valve collapse is a common missed diagnosis.
III
Post-Rhinoplasty Obstruction
Patients whose breathing was worse after prior rhinoplasty due to over-resection of supporting cartilage.
From the Patient Gallery
Nasal valve repair before & after photos.
A male patient in his 40s, documented in standardized studio conditions before and after nasal valve collapse treatment. Written photographic consent on file. Results vary by patient; this case is representative, not predictive.

Pre and post-operative comparison · Written consent on file
If this describes you, the next step is a quiet, unhurried conversation — not a sales call.
An Honest Note
When this operation may not be right for you.
Patients whose primary obstruction is from a deviated septum or enlarged turbinates benefit from septoplasty and turbinate reduction first.
Patients with primarily allergic obstruction benefit from optimised medical therapy first.
Patients whose dissatisfaction is driven primarily by mild discomfort that does not affect sleep or exertion may be reasonable to manage non-operatively.
Smokers should be counseled candidly about wound healing before any nasal surgery.
Static vs dynamic collapse
Nasal valve collapse is described as static or dynamic. Static collapse means the airway is narrow even at rest, often because the supporting cartilage is weak, displaced, or was reduced by prior surgery.
Dynamic collapse means the sidewall draws inward during inhalation, exercise, or sleep even when the airway looks adequate at rest. Many patients have a combination of both, and the examination is directed at identifying which pattern predominates.
03 · Approaches
Three paths to a stable nasal valve.
The internal and external nasal valves are the narrowest points of the airway. The right graft depends on which valve has collapsed and why — structural correction is what holds the airway open in the long term.
1 of 3 · Spreader Grafts
Compare your options
Surgery for a blocked nose, side by side
Different structures cause nasal obstruction, and each has a different operation. Select any two options to compare them directly, or open the full table below. The right choice is determined on examination.
What it addresses
Septoplasty: A deviated septum — the wall between the nostrils.
Turbinate Reduction: Enlarged inferior turbinates reducing airway space.
Changes appearance?
Septoplasty: No — purely functional.
Turbinate Reduction: No — internal only.
Incisions
Septoplasty: Hidden, inside the nostril. No external scar.
Turbinate Reduction: Inside the nose, tissue-preserving.
Typical anesthesia
Septoplasty: General or sedation, individualized.
Turbinate Reduction: Often combined with another nasal procedure.
General downtime
Septoplasty: Most desk work resumes within a few days.
Turbinate Reduction: Minimal; frequently done alongside septoplasty.
Insurance
Septoplasty: May be submitted for insurance review when medically necessary and when the patient's plan includes applicable out-of-network benefits.
Turbinate Reduction: May be submitted for insurance review when medically necessary and when the patient's plan includes applicable out-of-network benefits.
View full comparison table
| Attribute | Septoplasty | Turbinate Reduction | Nasal Valve Repair | Septorhinoplasty |
|---|---|---|---|---|
| What it addresses | A deviated septum — the wall between the nostrils. | Enlarged inferior turbinates reducing airway space. | Collapse or narrowing of the nasal valve (sidewall). | The septum and the external shape, together. |
| Changes appearance? | No — purely functional. | No — internal only. | Usually not; focus is structural support. | Yes — functional and cosmetic in one operation. |
| Incisions | Hidden, inside the nostril. No external scar. | Inside the nose, tissue-preserving. | Approach depends on the technique used. | Endonasal or a small columellar incision. |
| Typical anesthesia | General or sedation, individualized. | Often combined with another nasal procedure. | General or sedation, individualized. | General anesthesia, individualized. |
| General downtime | Most desk work resumes within a few days. | Minimal; frequently done alongside septoplasty. | Varies with the technique; discussed at consultation. | A splint for about a week; bruising settles over weeks. |
| Insurance | May be submitted for insurance review when medically necessary and when the patient's plan includes applicable out-of-network benefits. | May be submitted for insurance review when medically necessary and when the patient's plan includes applicable out-of-network benefits. | May be submitted for insurance review when medically necessary and when the patient's plan includes applicable out-of-network benefits. | The functional portion may be submitted for insurance review when medically necessary and when the plan includes out-of-network benefits; the cosmetic portion is self-pay. |
General information only. Anesthesia, downtime, and insurance vary by patient and plan and are determined individually at consultation.
04 · Anatomy
The two nasal valves, where breathing narrows.
The nose has two flow-limiting segments. The internal nasal valve sits higher, between the septum and upper lateral cartilage; the external nasal valve is the nostril opening itself. Understanding which valve is collapsing determines which repair is appropriate.
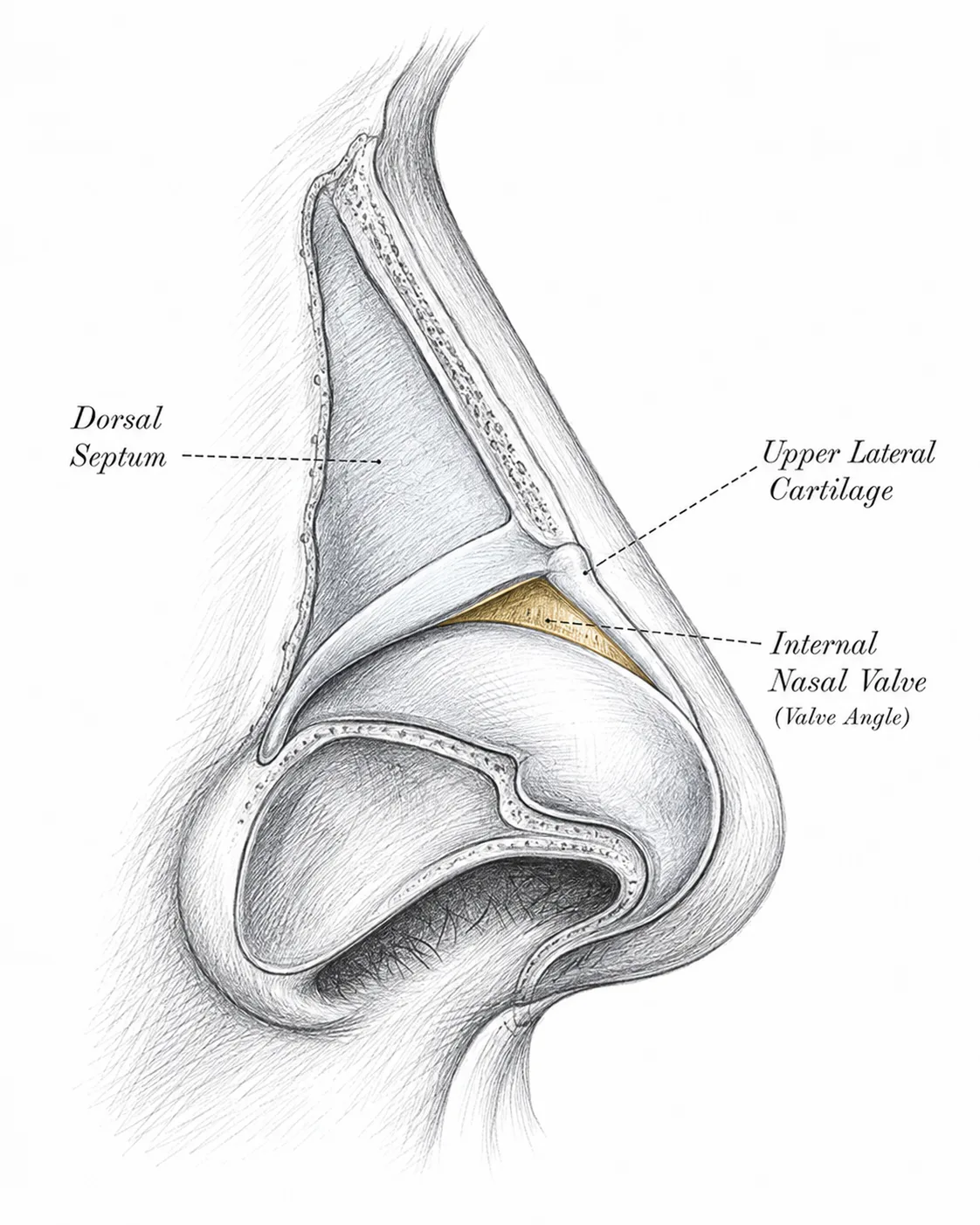
Internal nasal valve anatomy
The internal nasal valve is the narrow angle between the dorsal septum and upper lateral cartilage. Narrowing may be static, may worsen during inspiration, or may follow trauma, dorsal reduction, or prior rhinoplasty.
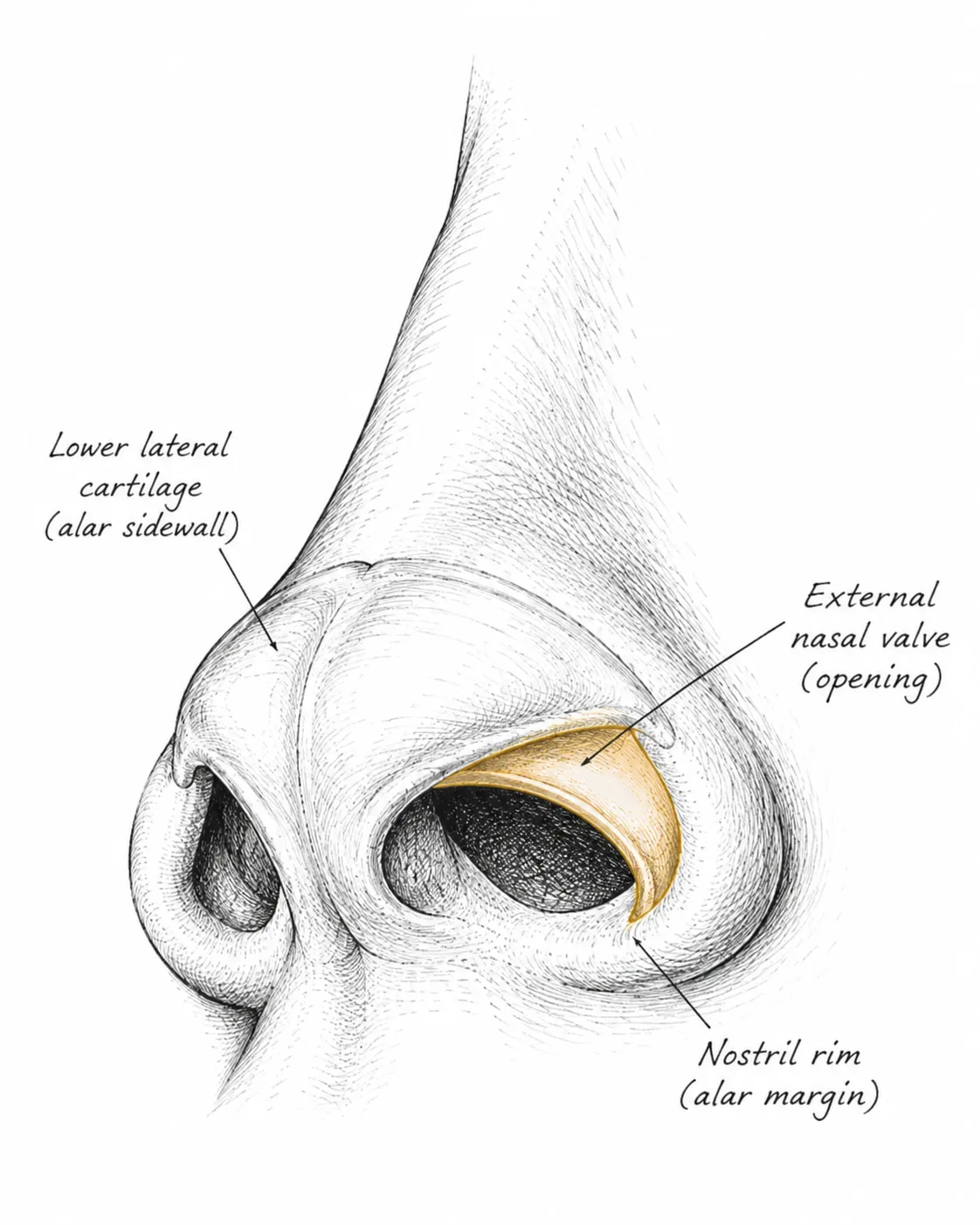
External nasal valve anatomy
The external nasal valve is the nostril opening itself. It is framed by the alar rim, the lateral crus of the lower lateral cartilage, the fibrofatty sidewall tissue, and the columella. Weak or malpositioned cartilage here lets the sidewall draw inward on inspiration.
Illustrative diagrams — stylized educational schematics, not patient images and not to scale.
05 · Technique
Nasal valve grafts for internal and external valve repair.
The internal valve, lower lateral cartilage, nostril rim, and broader sidewall are different zones. Each graft is placed in a different pocket, so the repair must follow the exact site of narrowing or collapse.
Internal Valve Support
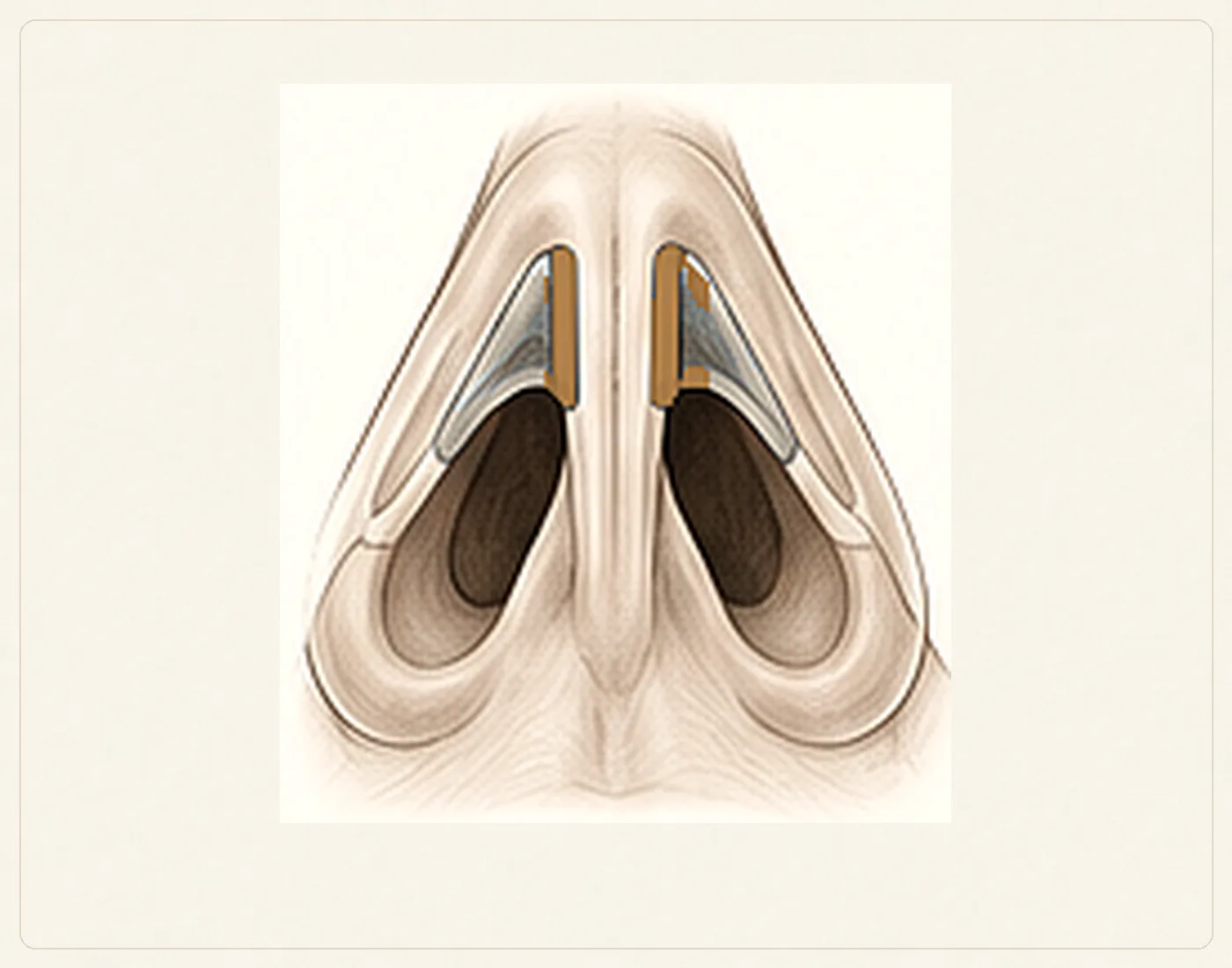
Spreader graft placement
Spreader grafts are placed between the dorsal septum and the upper lateral cartilages. They widen and stabilize the middle vault when internal-valve narrowing is the primary site of obstruction. They do not directly correct isolated rim weakness or broad lower-sidewall collapse.
External Valve Support
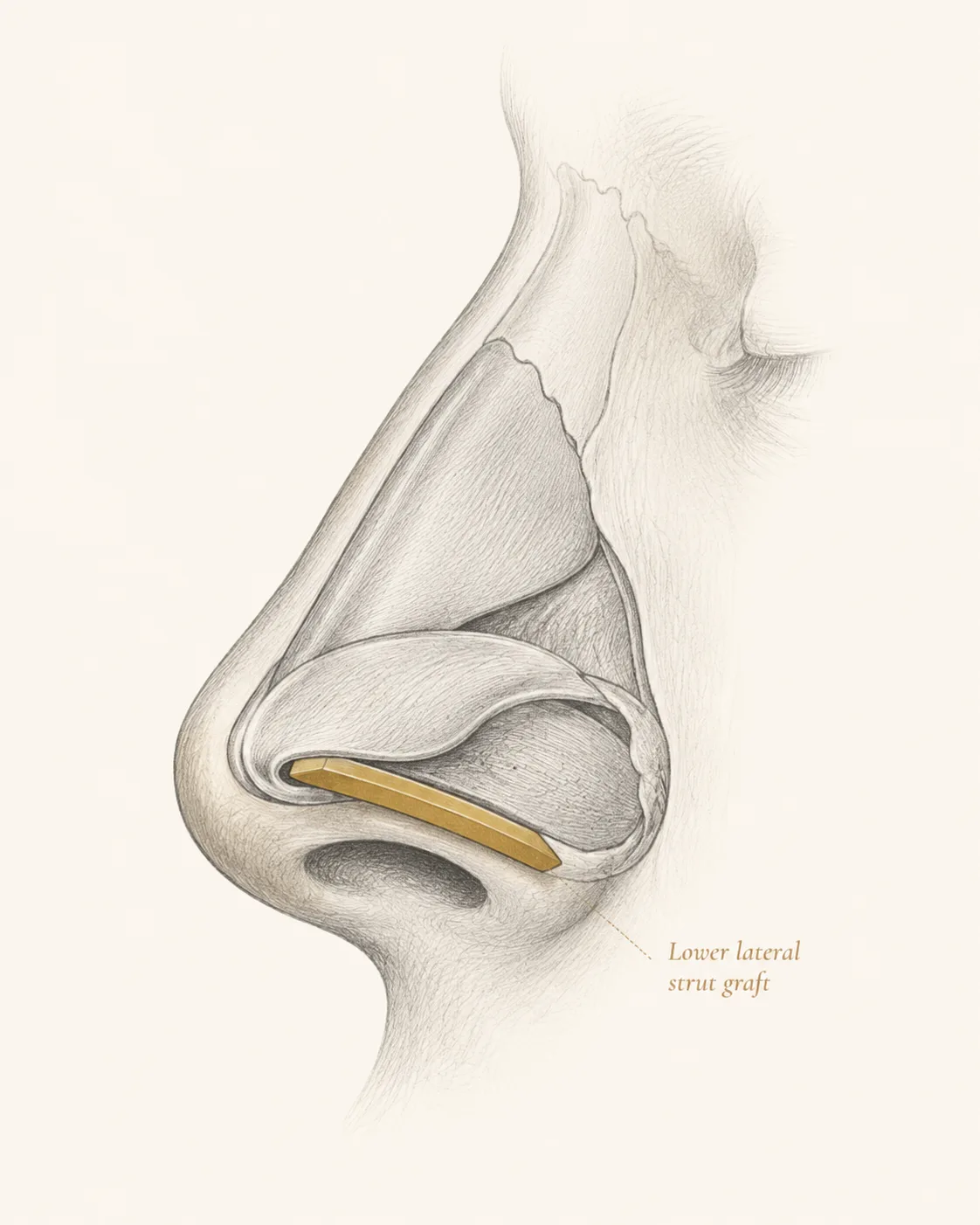
Lateral crural strut graft
A lateral crural strut graft is placed along the deep surface of the lateral crus. It reinforces or repositions weak, concave, over-resected, or malpositioned lower lateral cartilage and supports the external valve.
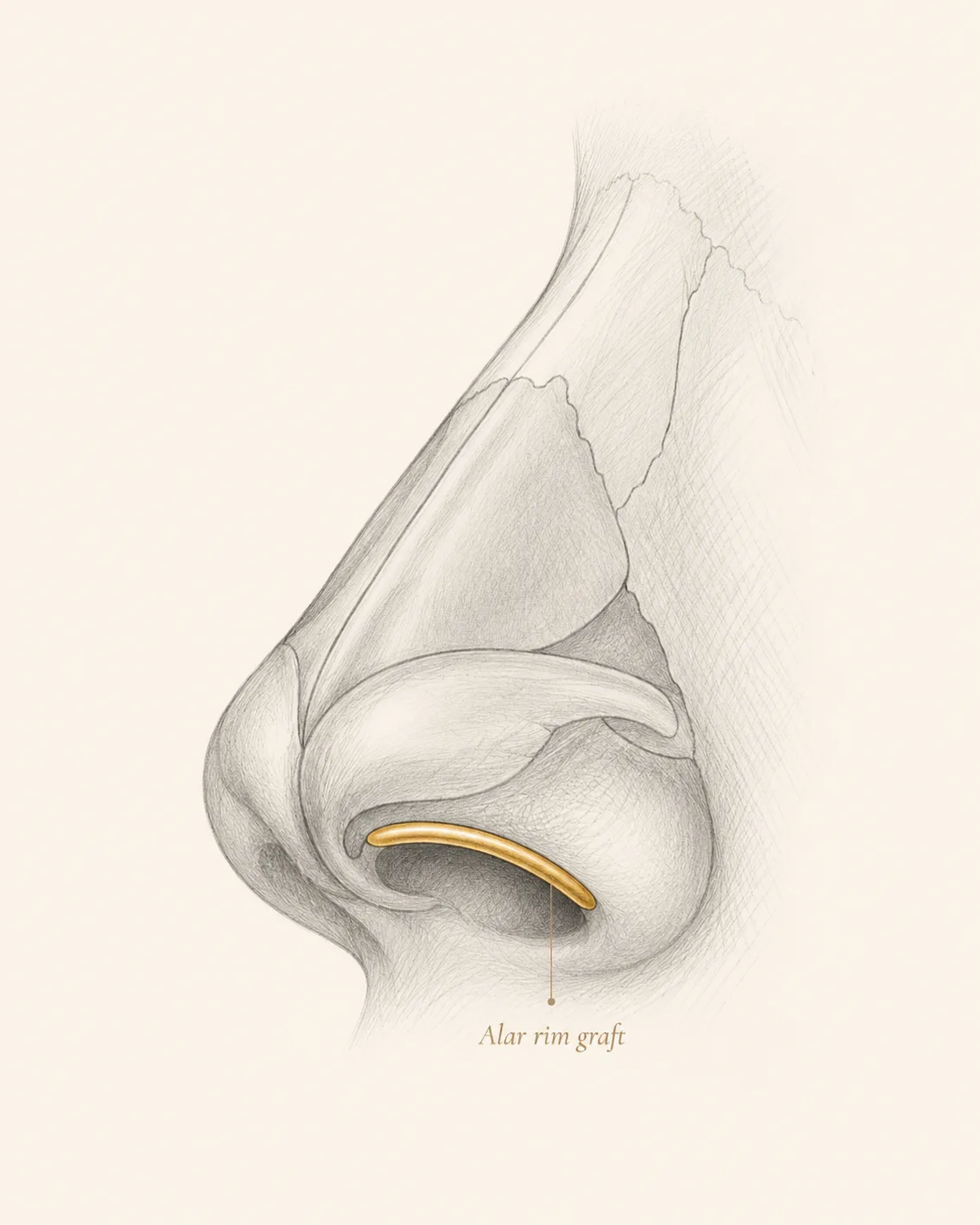
Alar rim graft
An alar rim graft is a slender cartilage graft placed in a precise pocket along the free margin of the nostril. It provides focused support for rim weakness, mild retraction, focal buckling, or loss of margin definition.
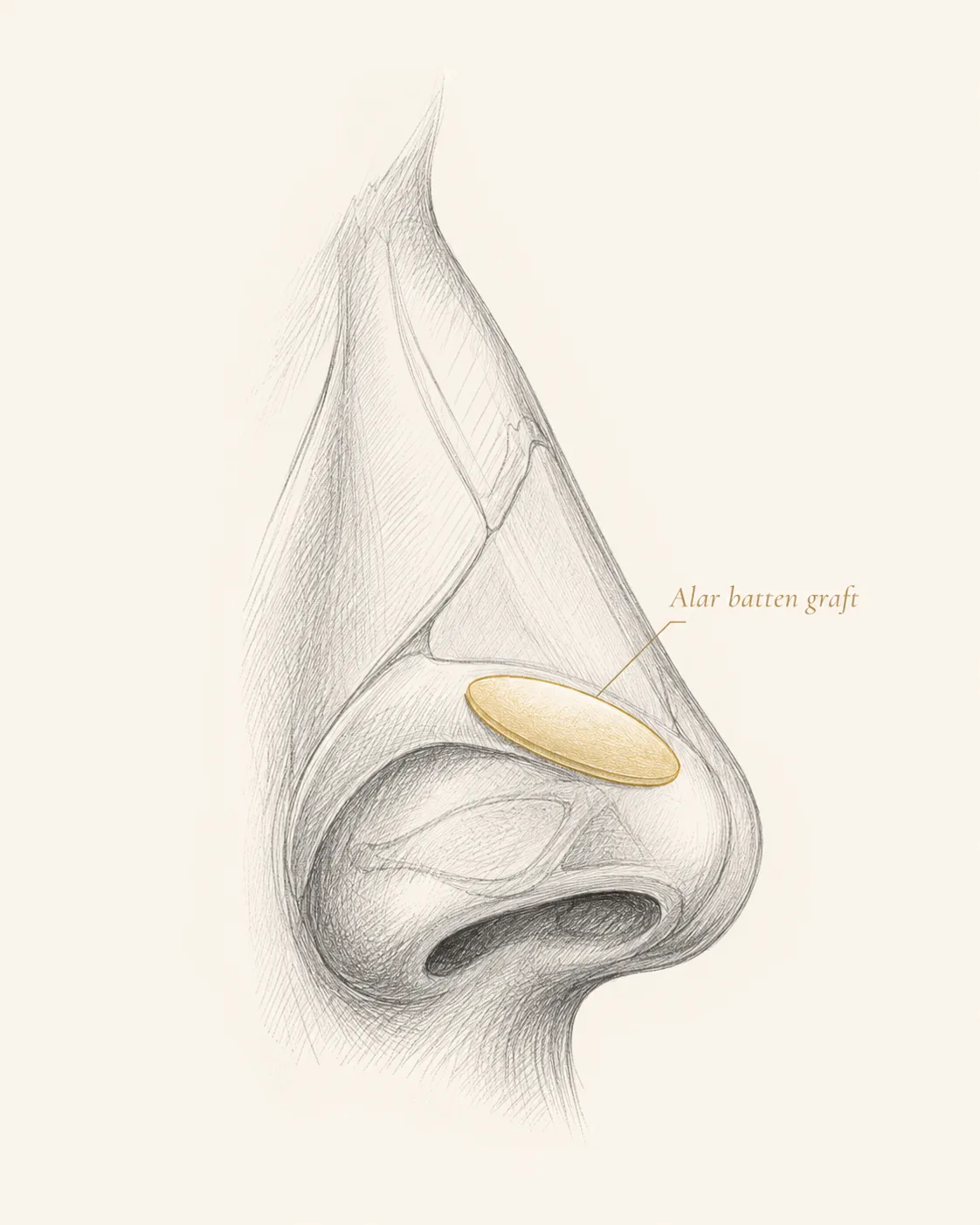
Alar batten graft
An alar batten graft is broader than a rim graft and is placed at the point of maximal lateral-wall weakness, commonly more lateral and cephalic to the alar margin. Depending on the pocket, it may support the external valve, intervalve region, or selected internal-sidewall weakness.
How the graft is selected
Dr. Mourad evaluates the epicenter of collapse, static versus dynamic narrowing, middle-vault width, lower lateral cartilage strength and position, septal deviation, turbinate size, prior surgery, trauma, donor-cartilage availability, and the desired external contour. Some patients need one site-specific graft; others need a combination because more than one zone contributes to obstruction.
Illustrative diagrams — stylized educational schematics, not patient images and not to scale. Some patients need one site-specific graft; a combination is used when more than one collapse zone contributes to obstruction.
At a Glance
Comparing treatment options for nasal valve collapse
Treatments range from temporary aids to minimally invasive options to structural reconstruction. The right choice depends on the pattern and severity of collapse found at examination, and this overview is educational — it does not replace a consultation.
| Option | Best suited for | Limitation | Type |
|---|---|---|---|
| Adhesive breathing strips | Quick at-home relief; a positive response is a useful diagnostic clue. | Temporary; works only while worn. | Temporary |
| Internal nasal dilators | Nighttime sidewall support; also a diagnostic clue. | Temporary; comfort and tolerance vary. | Temporary |
| Medical therapy (saline, steroid spray, allergy care) | When inflammation or allergy contributes to the obstruction. | Does not correct a structurally weak valve. | Medical |
| VivAer / temperature-controlled radiofrequency | Selected patients with limited, primarily dynamic lateral-wall weakness. | Not a substitute for grafting when cartilage deficiency is significant. | Minimally invasive |
| Latera absorbable implant | Lateral-wall support in selected dynamic weakness. | Absorbable; not for significant structural deficiency or complex revision. | Minimally invasive |
| Spreader grafts | Internal valve collapse at the mid-vault. | Requires surgery and donor cartilage. | Structural |
| Alar rim grafts | Focused support of the free nostril margin — rim weakness, mild retraction, or focal buckling. | Thin, site-specific graft; does not brace broad sidewall weakness. | Structural |
| Alar batten grafts | Placement-dependent bracing of the lateral wall at the zone of maximal weakness. | Requires surgery and a precise sidewall pocket. | Structural |
| Lateral crural strut grafts | Reinforcing or repositioning weak or malpositioned lower lateral cartilage — external valve support. | More complex than a single batten graft. | Structural |
| Lateral wall suspension sutures | Adjunct lateral-wall support in selected cases. | Less durable on their own when cartilage deficiency is significant. | Structural (adjunct) |
| Revision functional rhinoplasty | Collapse after prior surgery or cartilage over-resection. | Complex; often needs ear or rib cartilage. | Structural |
| Septoplasty / turbinate reduction | When a deviated septum or enlarged turbinates also contribute. | Addresses those causes, not the valve itself. | Structural (adjunct) |
Suitability depends on the pattern and severity of collapse found on examination. Minimally invasive options are not a substitute for structural grafting when cartilage support is significantly deficient.
Begin the conversation
A careful, honest evaluation is the right first step.
Cost, Financing & Insurance
Nasal Valve Collapse Treatment Cost, Financing & Insurance in NYC
The cost of nasal valve collapse treatment depends on the location and degree of valve weakness, whether the internal or external valve is involved, the technique selected, and whether the treatment is performed alone or with other nasal airway surgery.
MouradNYC is an out-of-network practice. Eligible medically necessary functional components may be submitted to insurance when the patient's plan includes applicable out-of-network benefits and plan requirements are met. Coverage, authorization, deductibles, coinsurance, allowed amounts, and patient responsibility vary by plan and are not guaranteed. Verification and authorization do not guarantee payment. Our office can help review benefits and guide patients through preauthorization when appropriate.
When pursuing coverage, insurers commonly look for a documented history of nasal obstruction, examination findings, the response to a Cottle or modified Cottle maneuver, a trial of medical therapy when inflammation is a factor, and a record of prior septoplasty if applicable. Photographs, endoscopy, or a NOSE score may also be requested, along with a clear distinction between the functional component and any elective cosmetic component, since only the functional portion is considered for coverage.
What May Affect Cost
- Internal vs external valve involvement
- Degree of valve weakness
- Repair technique used
- Whether grafting is required
- Whether combined with other nasal surgery
- Insurance plan requirements
This information is educational and is not a guarantee of pricing, insurance coverage, reimbursement, financing approval, or surgical candidacy. A personalized estimate is provided after consultation. Insurance coverage depends on the patient’s plan, medical necessity, documentation, and carrier requirements. Financing terms are determined by third-party financing providers.
06 · In Dr. Mourad's Words
Educational videos.
Short educational films and patient perspectives from the Manhattan practice.
Nasal Valve Collapse Surgery Explained
Dr. Mourad explains nasal valve collapse — how it is diagnosed and the surgical options for restoring nasal breathing.
Dr. Mourad in Practice
An overview of the practice and philosophy.
Patient Perspective
A patient discusses her experience before, during, and after surgery.
Inside the Consultation
How Dr. Mourad evaluates anatomy, goals, and candidacy.
07 · Recovery
What healing actually looks like.
Stage 01
First 1 – 7 Days
Early congestion and swelling are expected and can temporarily block airflow — this does not predict the final airway result. Nasal splints or internal packing, when used, are typically removed within one to seven days.
Stage 02
Weeks 1 – 2
Congestion and edema settle over the first one to two weeks. Saline care manages crusting, and the airway often still feels variable during this early phase.
Stage 03
Weeks 2 – 6
Many patients notice measurable breathing improvement between two and six weeks as swelling subsides. Strenuous exertion and nasal trauma are avoided for two to six weeks per surgeon-specific guidance.
Stage 04
Months 3 – 6
Graft support and structural remodeling stabilize over three to six months, when the final airway behavior becomes clear. Follow-up visits track healing across this period.
When to call the office
- Increasing one-sided pain, fever, or worsening redness or swelling.
- Heavy or persistent bleeding that does not settle with rest.
- A new bulge of the septum, or a sudden change in vision.
- Any symptom that worries you between scheduled visits.
Have a specific question?
Send a brief note describing your anatomy or concerns — the office will route it directly to Dr. Mourad for review.

Before You Arrive
Your consultation, prepared.
Bring photographs relevant to your concern, when available.
Bring records from any prior surgery, when available.
List current medications, supplements, and blood-thinning agents.
Note any prior anesthesia issues or chronic medical conditions.
Allow 60 minutes for the first consultation.
Bring questions; no decisions are made at the first visit.
Patient Reviews
Breathing & Nasal Airway Patient Experiences
Selected public reviews from patients treated for nasal obstruction and breathing concerns. Procedures differ by patient, and individual experiences are not a guarantee of outcome.
“I can now say I can breathe better than I ever have”
Real patient experiences
Selected public reviews from patients of the practice.
Your privacy matters
We never share personal health information.
Board-certified expertise
Dual board-certified facial plastic and reconstructive surgeon.
Individual results vary. Reviews reflect individual experiences and are not a guarantee of outcome.
At a Glance
Nasal valve repair fact snapshot.
- Treats
- Internal and external nasal valve collapse — sidewall weakness that restricts airflow, often after prior rhinoplasty, trauma, or with age.
- Does not treat
- Obstruction caused solely by a deviated septum, enlarged turbinates, polyps, or sinus disease — though these can be addressed in the same operation when present.
- Evaluation
- Examination of the valve at rest and during breathing, modified Cottle testing, and endoscopy when needed to map all contributors to obstruction.
- Related conditions
- Nasal valve collapse, deviated septum, chronic nasal obstruction, empty nose–type symptoms after over-resection.
- Possible combined procedures
- Septoplasty, turbinate reduction, functional or revision rhinoplasty, cartilage grafting.
- Recovery summary
- Most patients return to desk work in about a week; strenuous activity is limited for several weeks and breathing typically improves as swelling settles.
- Insurance / functional distinction
- Valve repair is a functional airway procedure and may be submitted for insurance review — coverage is never guaranteed. This out-of-network practice provides documentation for reimbursement.
- When to seek evaluation
- When nasal obstruction persists despite medical therapy or a prior septoplasty, or when the sidewall visibly collapses on inhalation.
Find your starting point
Which nasal breathing path fits your situation?
Answer three short questions to see which page explains the evaluation most relevant to you. This is educational orientation, not a diagnosis — a clinical examination is how the cause of nasal obstruction is actually determined.
Select an option for each question to see which page fits your situation.
This guide is general educational information, not medical advice or a diagnosis. Only an in-person examination can determine the cause of nasal obstruction and the appropriate treatment.
See all pathways
A combined revision evaluation likely fits
When both breathing and appearance are concerns after previous surgery, the anatomy is already altered and rebuilding structural support is often part of the plan. A revision evaluation looks at what the prior operation changed before anything is recommended.
A revision rhinoplasty conversation likely fits
Changing the appearance of a nose that has already had surgery is a different undertaking from a first operation, because scar tissue and prior changes shape what is possible. A revision evaluation is the right starting point.
A deviated-septum evaluation likely fits
Persistent, constant blockage that does not resolve with sprays or allergy treatment is often related to a deviated septum. Septoplasty is the functional operation that straightens the septum. If you have had prior nasal surgery, revision considerations also apply.
A nasal valve evaluation likely fits
When the side of the nose draws inward on hard inspiration, the nasal valve — the narrowest part of the airway — may be the contributor rather than the septum alone. This is assessed directly on examination.
A turbinate and sinus evaluation likely fits
Congestion that fluctuates with colds, allergies, or facial pressure often involves swollen turbinates or the sinuses rather than the septum by itself. The evaluation looks at the whole airway before any procedure is considered.
A septorhinoplasty conversation likely fits
When breathing and appearance are both concerns, they can often be addressed together in a single planned operation — straightening the septum while refining the external shape — so there is one recovery rather than two.
A rhinoplasty conversation likely fits
When the concern is the shape of the nose, rhinoplasty is the operation that refines it. A consultation focuses on your goals and whether the underlying anatomy supports them.
A revision evaluation likely fits
After previous nasal surgery, a fresh structural evaluation is the right starting point because the anatomy has already been changed once.
Start with a functional nasal evaluation
Your answers point to more than one possible contributor, which is common. A functional nasal examination is how the cause is identified before any treatment is considered.
Why patients trust this practice
Care led by a double board-certified specialist
Double board certified
American Board of Facial Plastic & Reconstructive Surgery and American Board of Otolaryngology — Head & Neck Surgery.
AAFPRS Fellowship Director
Trains fellows through the American Academy of Facial Plastic and Reconstructive Surgery.
Published author
Contributions to the academic literature of facial plastic surgery.
Face, nose & sinus focus
A practice concentrated above the clavicles, including complex revision evaluations.
Frequently Asked
Patient questions, honestly answered.
Nasal valve collapse refers to failure of the internal or external valve structures that normally resist inward movement during inspiration, producing dynamic airflow obstruction. A deviated septum is a displacement of the central septal cartilage or bone that narrows one nasal airway statically. Both can coexist and contribute to symptoms, but the physical exam maneuvers and visual findings differ: valve collapse is often evident with inspiratory wall movement while septal deviation is visible as a midline shift or lateral displacement. Definitive treatment decisions require an in-person assessment to determine whether valve reconstruction, septoplasty, or both are indicated.
Patients with valve-related obstruction commonly report difficulty drawing air through the nose, nasal flaring with effort, or intermittent improvement when manually supporting the sidewall. In the office, the surgeon will observe inspiratory collapse at rest or with forced inspiration and may use maneuvers such as the modified Cottle to reproduce symptom relief. Nasal endoscopy can document dynamic collapse and rule out intranasal lesions. Objective testing such as rhinomanometry or acoustic rhinometry can supplement the exam but do not replace the targeted clinical assessment.
Diagnosis is primarily clinical: careful inspection during quiet and deep inspiration, palpation of lateral wall mobility, and the Cottle or modified Cottle maneuvers are central. Nasal endoscopy under topical anesthesia helps evaluate the internal airway and identify additional causes of obstruction. In selected cases, rhinomanometry, acoustic rhinometry, or imaging help quantify obstruction or reveal concurrent problems but may miss dynamic collapse. A comprehensive diagnosis integrates symptoms, exam findings, and adjunctive tests to define which anatomic zone requires repair.
Initial management includes medical therapy for reversible contributors: topical nasal steroids for mucosal inflammation and saline irrigation for mucociliary clearance. External dilators, internal adhesive stents, and short-term intranasal devices can provide symptomatic relief and serve as a diagnostic trial for valve-related benefit. These measures are appropriate when inflammation is present or as temporizing options, but persistent mechanical collapse despite conservative care usually warrants surgical consideration. The decision to operate depends on symptom burden, exam findings, and response to these non-surgical trials.
Internal-valve narrowing at the middle vault is commonly treated with spreader grafts placed between the dorsal septum and upper lateral cartilages. External-valve repair is site-specific. A lateral crural strut graft reinforces or repositions the lower lateral cartilage; an alar rim graft supports the free nostril margin; and an alar batten graft braces a broader weak segment of the lateral wall. Some patients need one site-specific technique, while a combination is used when more than one collapse zone is present.
Common sources of structural grafts are septal cartilage, auricular (ear) cartilage, and costal (rib) cartilage when greater volume or strength is required. Septal cartilage is preferred when available because it is locally situated and avoids a separate incision; auricular cartilage is useful when septal tissue is insufficient and provides a curved graft for alar support. Rib cartilage is reserved for extensive reconstructions, such as severe post-rhinoplasty collapse or saddle deformity, when more robust material is necessary. Choice of donor site is individualized based on prior surgery, the volume of graft needed, and the reconstructive goals discussed during consultation.
The endonasal approach uses internal incisions and is appropriate for limited graft placement or small structural adjustments with preserved tip exposure. An open approach provides wide bilateral exposure of the middle vault and tip and is chosen when complex grafting, multizonal reconstruction, or revision surgery is anticipated. Open exposure facilitates precise graft shaping and placement but involves a small transcolumellar incision; endonasal techniques avoid external incision but can limit visibility in complex cases. Dr. Mourad selects the approach that best balances exposure, graft control, and the patient’s prior operative history.
Early postoperative congestion and edema are expected for 1–2 weeks and are not predictive of final airway outcome. Many patients notice measurable breathing improvement within 2–6 weeks as swelling subsides, but structural remodeling and final airway behavior often evolve over 3–6 months. Nasal splints or internal packing, when used, are typically removed within 1–7 days depending on the procedure. Activity restrictions are conservative: avoid strenuous exertion and nasal trauma for 2–6 weeks and follow surgeon-specific return-to-work guidelines discussed at the visit.
Risks include persistent or recurrent obstruction, asymmetry of the external nose, graft visibility or irregularity, infection, and donor-site morbidity when autologous cartilage is harvested. Over- or undercorrection of lateral wall position can necessitate revision in some cases. General surgical risks such as bleeding and anesthesia-related events also apply. A frank discussion of these possibilities and the contingency plan for revision—should it become necessary—is part of the preoperative consultation.
Prior rhinoplasty often alters native cartilage availability and the relationship between the middle vault and tip, making valve repair more complex. Scar tissue and previous grafts may limit options and require alternative donor sites such as ear or rib cartilage. Revision valve repair typically requires more extensive exposure and precise grafting to recreate lost support rather than simple maneuvers used in primary cases. Dr. Mourad outlines these differences during consultation and explains the staged options and realistic expectations for revision reconstruction.
Static collapse means the airway is narrow even at rest, often because the supporting cartilage is weak, displaced, or was reduced by prior surgery. Dynamic collapse means the sidewall draws inward during inhalation, exercise, or sleep even when the airway looks adequate at rest. Many patients have a combination of both, and the examination is directed at identifying which pattern predominates. Temporary improvement with an adhesive breathing strip or an internal nasal dilator can be a useful clue that the valve is contributing, though it does not by itself determine whether surgery is appropriate.
Minimally invasive options are part of the broader treatment landscape and can help selected patients with limited, primarily dynamic lateral-wall weakness. Latera is an absorbable implant placed to support the lateral wall, and radiofrequency techniques such as VivAer remodel soft tissue of the nasal valve in carefully chosen candidates. They are not a substitute for structural grafting when there is significant cartilage deficiency, prior over-resection, saddle deformity, complex revision anatomy, or collapse involving more than one zone. Insurance coverage for these options varies, and whether they are suitable depends entirely on the anatomy found at examination.
Nasal valve repair is performed in an accredited surgical facility, and the setting and anesthesia are selected for the complexity of the planned reconstruction and the patient's overall health. Limited grafting may be done under local anesthesia with sedation, while more extensive or combined reconstruction is typically performed under general anesthesia. Operative time varies with the number of valves treated, the grafts required, and whether septoplasty, turbinate reduction, or rhinoplasty are combined in the same operation. Most functional valve procedures are same-day, with discharge once standard recovery criteria are met; the specific plan is reviewed in advance.
It can be. Persistent obstruction after septoplasty is a common reason valve collapse is eventually identified, because septoplasty corrects the septum but does not address a weak or collapsing sidewall. After rhinoplasty, breathing can be worse when supporting cartilage was over-resected, the middle vault narrowed, or the lower lateral cartilages were weakened. These situations often require structural grafting — sometimes using ear or rib cartilage — to rebuild lost support rather than the simpler maneuvers used in first-time surgery. A focused examination determines whether the valve, the septum, the turbinates, or a combination is responsible.
Because nasal valve repair treats nasal obstruction, it may be covered when it is medically necessary, though coverage always depends on the individual plan. Insurers commonly look for a documented history of nasal obstruction, examination findings, the response to a Cottle or modified Cottle maneuver, and a trial of medical therapy when inflammation is a factor. They may also request photographs or endoscopy, a NOSE (Nasal Obstruction Symptom Evaluation) score when used, a record of prior septoplasty if applicable, and a clear distinction between the functional and any cosmetic components of the plan. Our office can help review benefits and assist with preauthorization where appropriate.
Nasal valve repair can be performed as a standalone procedure or together with septoplasty, turbinate reduction, or sinus surgery when more than one structure contributes to obstruction. Septoplasty and turbinate reduction address the septum and turbinates and are not substitutes for treating true valve dysfunction. When the valve is the problem, it has to be supported directly, which is the role of structural grafting. The decision to address one structure or several is based on the examination and on which contributors are actually present.
Clinical references
This page draws on published clinical practice guidelines and public-health references. These sources inform general patient education and do not replace an individual evaluation with Dr. Mourad.
- 01Rhee JS, Weaver EM, Park SS, et al. Clinical Consensus Statement: Diagnosis and Management of Nasal Valve Compromise. Otolaryngology–Head and Neck Surgery. 2010;143(1):48–59. AAO-HNSF consensus (nasal valve)
- 02American Academy of Otolaryngology–Head and Neck Surgery Foundation. Clinical Consensus Statement: Septoplasty with or without Inferior Turbinate Reduction. Otolaryngology–Head and Neck Surgery. 2015;153(5):708–720. AAO-HNSF consensus
- 03U.S. National Library of Medicine (MedlinePlus). Nose Injuries and Disorders. MedlinePlus
- 04American Academy of Otolaryngology–Head and Neck Surgery. Position Statement: Nasal Valve Repair. Approved 2023. AAO-HNS position statement
- 05American Rhinologic Society. Position Statement: Nasal Valve Collapse. American Rhinologic Society
- 06Kandathil CK, Spataro EA, Laimi K, Moubayed SP, Most SP, Saltychev M. Repair of the Lateral Nasal Wall in Nasal Airway Obstruction: A Systematic Review and Meta-analysis. JAMA Facial Plastic Surgery. 2018;20(4):307–313. JAMA Facial Plast Surg (meta-analysis)
- 07Silvers SL, et al. Temperature-controlled radiofrequency device treatment of the nasal valve for nasal airway obstruction (VATRAC): a randomized controlled trial. International Forum of Allergy & Rhinology. 2021. Int Forum Allergy Rhinol (VivAer/TCRF RCT)
- 08Stolovitzky P, Sidle DM, Ow RA, Nachlas NE, Most SP. A prospective study for treatment of nasal valve collapse due to lateral wall insufficiency: outcomes using a bioabsorbable implant. Laryngoscope. 2018;128(11):2483–2489. Laryngoscope (Latera implant)
- 09André RF, Paun SH, Vuyk HD. Endonasal spreader graft placement as treatment for internal nasal valve insufficiency: no need to divide the upper lateral cartilages from the septum. Archives of Facial Plastic Surgery. 2004;6(1):36–40. Arch Facial Plast Surg (spreader graft / internal valve)
- 10Gunter JP, Friedman RM. Lateral crural strut graft: technique and clinical applications in rhinoplasty. Plastic and Reconstructive Surgery. 1997;99(4):943–952. Plast Reconstr Surg (lateral crural strut graft)
- 11Ellenbogen R, Bazell G. Nostrilplasty: raising, lowering, widening, and symmetry correction of the alar rim. Aesthetic Surgery Journal. 2002;22(3):227–237. Aesthet Surg J (alar rim)
- 12Toriumi DM, Josen J, Weinberger M, Tardy ME Jr. Use of alar batten grafts for correction of nasal valve collapse. Archives of Otolaryngology–Head & Neck Surgery. 1997;123(8):802–808. Arch Otolaryngol Head Neck Surg (alar batten graft)
Continue Reading
Related nasal airway care
Nasal valve collapse often sits alongside other structural causes of obstruction. These related pages explain the conditions and procedures most often considered together.
Revision Rhinoplasty
When breathing is worse after a prior rhinoplasty that weakened or over-resected support.
Read moreSeptoplasty
Correction of a deviated septum, when the septum itself is the obstructing problem.
Read moreTurbinate Reduction
When enlarged turbinates also contribute to nasal obstruction.
Read moreSeptorhinoplasty
Combined functional and structural surgery of the septum and nose.
Read moreNasal Valve Collapse (condition)
The underlying condition explained — causes, symptoms, and how it is diagnosed.
Read moreDeviated Septum (condition)
A common, separate cause of one-sided nasal blockage.
Read moreThe Most Important Step
Your expert consultation.
A careful evaluation by a double board-certified physician is the right first step. The conversation is unhurried, the diagnosis is honest, and the operative plan is built around what your anatomy can sustain and what you actually want.