Double Board Certified · Functional Sinus Care
Acute Sinusitis — most cases resolve; some require more.
Acute sinusitis is inflammation of the sinuses lasting less than four weeks — most commonly viral, occasionally bacterial. The right management depends on…
ABFPRS
Facial Plastic & Reconstructive Surgery
ABOto
Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
In Consultation
"The most important question in acute sinusitis is when antibiotics are actually needed — and when they are not."
A Note from Dr. Mourad
"Acute sinusitis is inflammation of the sinuses lasting less than four weeks — most commonly viral, occasionally bacterial. The right management depends on duration, severity, and the trajectory of symptoms."
— Dr. Moustafa Mourad, MD
Overview
What is acute sinusitis?
Acute sinusitis is an inflammation of the lining of one or more of the paranasal sinuses that lasts less than four weeks. Most cases begin as a viral upper-respiratory infection; a smaller proportion progress to a bacterial infection when sinus drainage is blocked and secretions become trapped behind a swollen sinus opening.
It produces facial pressure or pain, nasal obstruction, thick discolored nasal discharge, post-nasal drip, reduced sense of smell, and sometimes fever or dental pain. Symptoms are concentrated over the affected sinuses — the cheeks, between or behind the eyes, or the forehead.
Most episodes resolve with supportive care: saline irrigation, decongestants, nasal steroid sprays, and time. Antibiotics are reserved for cases that meet specific bacterial criteria. Recurrent or prolonged episodes warrant evaluation for an underlying anatomic or inflammatory driver.
Key takeaways
- Acute sinusitis is sinus inflammation lasting less than four weeks.
- Most cases are viral and self-limited; a smaller share are bacterial.
- Supportive care — saline rinses, decongestants, nasal steroids, and time — resolves most episodes.
- Antibiotics are reserved for cases that meet specific bacterial criteria.
- Recurrent or prolonged episodes warrant evaluation for an underlying driver.
An Established Academic Authority
Double board certification. Fellowship director. Published author. A surgeon's surgeon.
ABFPRS
Board Certified
American Board of Facial Plastic & Reconstructive Surgery
ABOto
Board Certified
American Board of Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
American Academy of Facial Plastic and Reconstructive Surgery
Textbook
Published Author
Contributions to the academic literature of facial plastic surgery
Dual board certification in both Facial Plastic & Reconstructive Surgery and Otolaryngology — Head & Neck Surgery.
Castle Connolly Top Doctor — Plastic Surgery, 202602 · Symptoms
How this condition typically presents.
Three patterns are most common. Patients often recognise themselves in one or more of these.
I
Facial Pressure & Pain
Localised pressure or pain over the affected sinus — most commonly the cheek, forehead, or between the eyes.
II
Nasal Obstruction & Discharge
Thick nasal discharge, congestion, and reduced sense of smell, often with post-nasal drip.
III
Systemic Symptoms
Fever, fatigue, and worsening symptoms after initial improvement — a pattern that may suggest bacterial infection.
03 · Anatomy
Viral vs bacterial sinusitis.
The distinction matters because the treatment is different. Most acute sinusitis is viral and self-limited; a smaller proportion is bacterial and benefits from antibiotics.
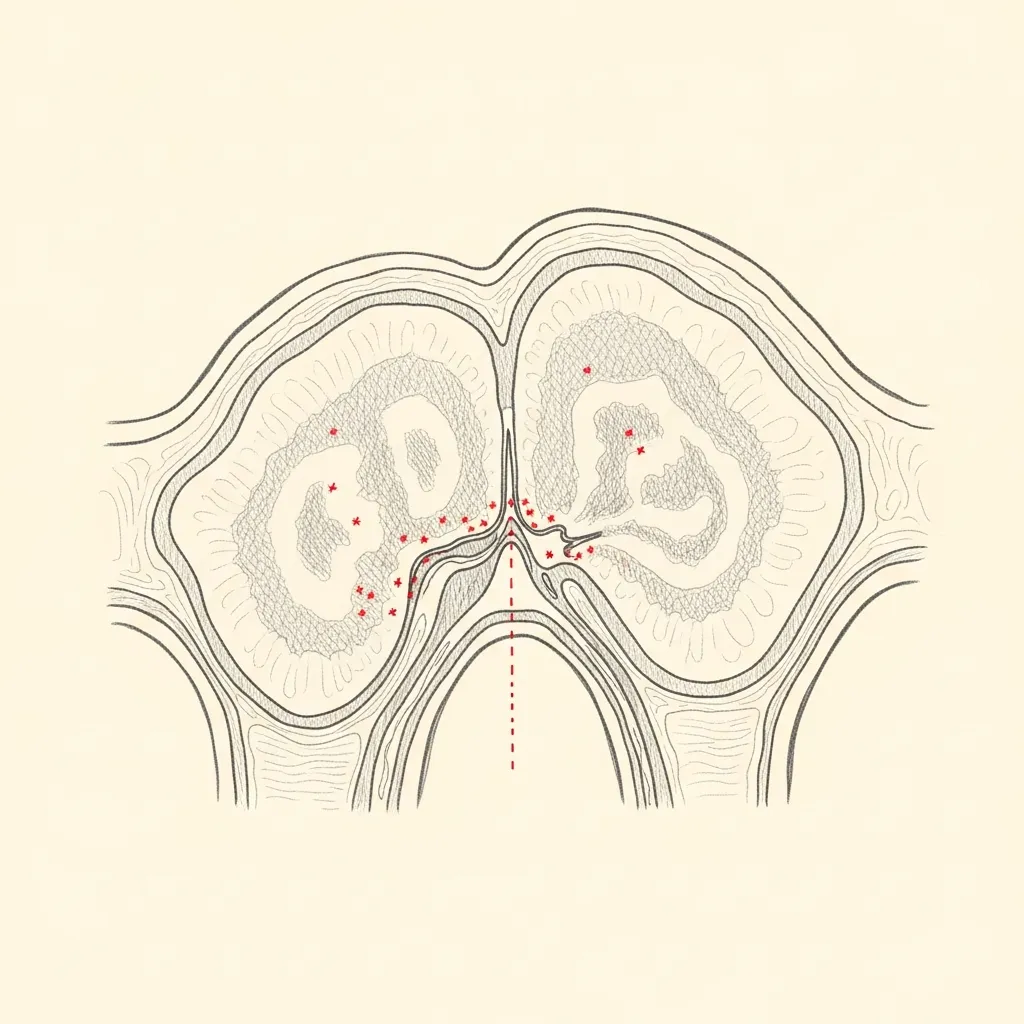
Viral
The common pattern
Viral sinusitis is the most common form — symptoms peak in the first 3 to 5 days and steadily improve thereafter. Antibiotics are not indicated.
Supportive care — saline irrigation, hydration, rest, and selective use of decongestants — is the right management for the typical case.
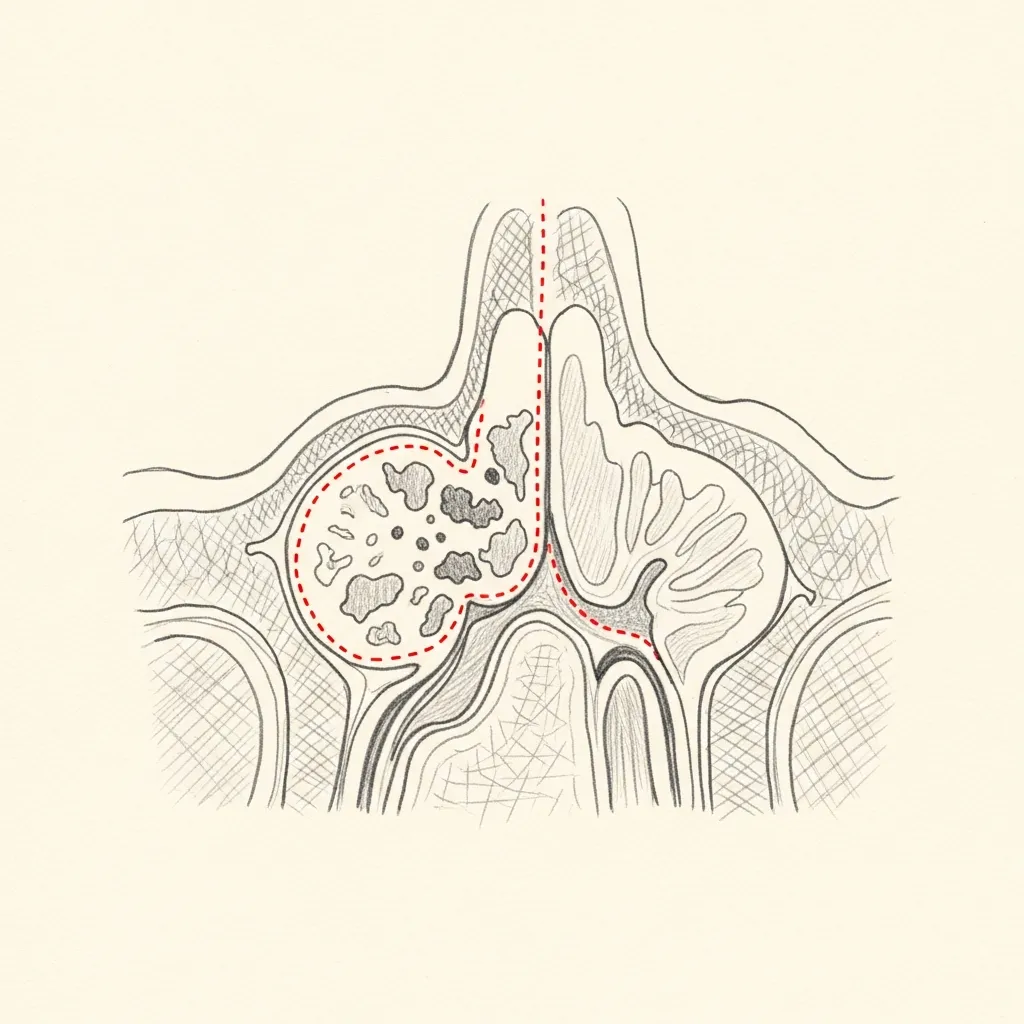
Bacterial
When antibiotics are appropriate
Bacterial sinusitis typically presents with one of three patterns: symptoms persisting beyond 10 days without improvement, severe symptoms with fever and purulent discharge, or initial improvement followed by worsening.
When the clinical pattern fits, a targeted antibiotic course is appropriate; broad-spectrum coverage is reserved for specific situations.
Illustrative diagrams. The clinical distinction guides treatment, not imaging alone.
04 · Diagnosis
How the diagnosis is made.
Diagnosis is clinical for most cases — symptom duration, character, and trajectory are the key variables.
Nasal endoscopy is performed when symptoms are atypical, prolonged, or recurrent.
Imaging is reserved for suspected complications or cases that have not responded to appropriate therapy.
05 · Treatment Options
Treatments matched to the diagnosis.
Treatment is individual. The right answer ranges from optimised medical therapy to a focused procedure to definitive surgery.
Medical Therapy
Saline irrigation, topical decongestants, intranasal steroids, and selective use of antibiotics.
Learn More
Balloon Sinuplasty
For recurrent acute sinusitis when imaging shows correctable outflow obstruction.
Learn More
Endoscopic Sinus Surgery
Reserved for complicated, recurrent, or treatment-refractory cases.
Learn More
01 · Why Dr. Mourad
Diagnosis first, treatment second.
Dr. Mourad approaches acute sinusitis with a clear diagnostic framework — viral versus bacterial, uncomplicated versus complicated — to avoid the over-prescription of antibiotics.
In-office evaluation including nasal endoscopy clarifies the cause; imaging is reserved for cases that warrant it.
When antibiotics are appropriate, they are prescribed deliberately; when they are not, the conversation about supportive care is just as deliberate.
When to Seek Care
When to seek care promptly.
Severe facial pain, high fever, or visual changes — these warrant urgent evaluation.
Significant facial swelling or redness around the eye — evaluate immediately.
Severe headache, neck stiffness, or change in mental status — evaluate immediately.
Symptoms not responding to appropriate therapy within 5 to 7 days — return for re-evaluation.
Outlook
What to expect.
When the diagnosis is correct and the right treatment is applied, the outlook is generally good. Most patients describe meaningful improvement in symptoms and day-to-day function.
When symptoms persist despite treatment, the workup is re-opened. Persistent symptoms with no answer almost always mean the diagnosis is incomplete.

Living Well
Day-to-day measures that help.
Daily saline irrigation, control of indoor allergens, and good sleep hygiene meaningfully reduce day-to-day symptoms for many patients.
Medical therapy, when prescribed, works best when used consistently rather than as needed — this is one of the most common reasons treatment seems to fail.
Frequently Asked
Patient questions, honestly answered.
Acute sinusitis is symptomatic inflammation of the paranasal sinuses that typically lasts up to four weeks. Most episodes begin after a viral upper respiratory infection and improve within 7–10 days. Symptoms that persist beyond 10 days or follow a pattern of initial improvement and then worsening suggest possible bacterial infection. Final diagnosis and management require clinical assessment and, when helpful, office nasal endoscopy.
Distinguishing viral from bacterial sinusitis is based on symptom trajectory rather than a single test. Viral illness usually improves by day 7–10; bacterial infection is more likely with symptoms lasting longer than 10 days, a severe onset (high fever with purulent drainage), or a double‑worsening pattern after initial improvement. Nasal endoscopy can show focal purulence or an occluded ostium and often changes management. In-person evaluation is necessary before starting antibiotics.
Antibiotics are reserved for patients who meet guideline-based criteria: severe symptoms at onset, symptoms lasting longer than 10 days without improvement, or a double‑worsening pattern. Recent antibiotic exposure, penicillin allergy, and prior culture results also inform agent selection. In many uncomplicated acute cases, symptomatic therapies and topical measures are appropriate. Decisions about antibiotics should follow in-person assessment and stewardship principles.
The core office rhinologic assessment is a focused history and nasal endoscopy to inspect the ostiomeatal complex, detect purulence, and evaluate mucosal edema or polyps. Endoscopic findings frequently change management by localizing disease. CT imaging is reserved for complicated presentations, failure of medical therapy, or procedural planning. Cultures taken endoscopically are used selectively for refractory or severe infections needing targeted therapy.
Yes. Allergic inflammation causes mucosal swelling that narrows sinus ostia and impairs ventilation and drainage. Structural issues such as a deviated septum, turbinate hypertrophy, or obstructing polyps create focal mechanical blockage. Evaluation includes allergy history, targeted endoscopy, and selective testing. Treating both inflammatory drivers and correctable structural contributors reduces the risk of recurrence.
See a sinus specialist when symptoms are severe, prolonged beyond 10 days, recurrent, or not responding to guideline-based medical therapy. Early referral is appropriate for visual symptoms, suspected complications, or when structural contributors are suspected. A rhinologist can perform office nasal endoscopy and plan selective imaging or procedural options. In-person specialist assessment clarifies candidacy for interventions such as balloon sinuplasty or FESS.
Nasal endoscopy provides direct visualization of the middle meatus and ostiomeatal complex, allowing identification of localized purulence, mucosal edema, polyps, or obstructing anatomy. These findings often alter treatment decisions by pinpointing where drainage is impaired. Endoscopy can also guide culture collection in refractory cases and refine procedural planning. It is performed in office under topical anesthesia and typically adds minimal time to the visit.
Procedural treatment is considered when recurrent or refractory episodes are driven by identifiable structural obstruction or when medical therapy fails despite adherence. Balloon sinuplasty is best for isolated ostial narrowing without significant polyp disease or bony pathology. FESS is indicated for more extensive disease, polyp burden, or when adjunctive procedures like septoplasty or turbinate reduction are required. Final candidacy requires endoscopic evaluation and, when useful, CT imaging.
Recovery varies by procedure but typically includes brief nasal congestion, crusting, and intermittent bloody drainage for several days to a few weeks. Follow-up visits involve endoscopic cleaning and topical irrigation to promote mucosal healing. Most patients resume light activity within 24–72 hours, with gradual return to normal exertion over one to two weeks depending on the procedure. Specific postoperative instructions and timelines are reviewed during in-person consultation.
Reducing recurrence requires addressing both inflammatory and structural drivers. Measures include regular saline irrigations, appropriate topical intranasal steroids for inflammatory disease, allergy management when indicated, smoking cessation, and treatment of obstructing anatomy if present. Optimizing nasal hygiene and following postoperative care instructions after any procedure also help. Discuss a personalized prevention plan during specialist evaluation.
Urgent evaluation is required for visual changes, new or worsening eye pain, eyelid swelling, double vision, neurologic symptoms, or severe headache with fever. These signs may indicate orbital or intracranial complications and require immediate imaging and hospital‑based management. Rapidly progressive systemic symptoms also warrant prompt attention. For routine sinus symptoms without these red flags, schedule timely outpatient specialist care.
CT imaging is not routinely required for a typical uncomplicated acute sinus infection expected to resolve with medical therapy. CT is reserved for complicated cases, atypical presentations, recurrent disease, or when planning procedures. Endoscopy often guides the need for imaging by localizing disease. Imaging decisions are made during in-person evaluation to minimize unnecessary radiation.
Continue Reading
Related sinus care
Chronic Sinusitis Treatment
When sinus inflammation persists beyond twelve weeks.
Read moreRecurrent Sinus Infections
Evaluation when infections keep returning.
Read moreSinus Surgery
Endoscopic and balloon options for refractory disease.
Read moreDo I Need Sinus Surgery?
A plain-language guide to when surgery is considered.
Read moreThe Most Important Step
Get an expert evaluation.
A careful evaluation by a double board-certified physician is the right first step. The conversation is unhurried, the diagnosis is honest, and treatment is matched to what you actually have.