Double Board Certified · Male Aesthetics
Male Buccal Fat Removal — sex-specific aesthetic considerations.
Buccal fat removal in men is a different conversation than in women. The lower face is broader, the bone is heavier, and over-thinning produces a gaunt look…
ABFPRS
Facial Plastic & Reconstructive Surgery
ABOto
Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
In Consultation
"The masculine lower face tolerates very little reduction. A small change in the mirror is the right size of change."
A Note from Dr. Mourad
"Buccal fat removal in men is a different conversation than in women. The lower face is broader, the bone is heavier, and over-thinning produces a gaunt look that ages poorly. The right operation is conservative, well-staged, and individually evaluated."
— Dr. Moustafa Mourad, MD
Overview
What is male buccal fat removal?
Male buccal fat removal is a small intraoral procedure that reduces a portion of the buccal fat pad in the lower cheek to add definition to the mid-face and jawline. In men, the goal is typically angular contour and a clearer demarcation between the cheek and jaw — not the high-hollow look often pursued in other patients.
It is considered when persistent lower-cheek fullness softens the jawline at a normal weight, and when examination shows the fullness is anatomically due to the buccal pad rather than overall facial fat, prominent masseter, or skin laxity.
Conservative volume removal matters even more in male contouring. Over-resection produces a gaunt mid-face that does not age well; the aim is restraint, with the operation matched to long-term facial structure rather than a short-term trend.
An Established Academic Authority
Double board certification. Fellowship director. Published author. A surgeon's surgeon.
ABFPRS
Board Certified
American Board of Facial Plastic & Reconstructive Surgery
ABOto
Board Certified
American Board of Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
American Academy of Facial Plastic and Reconstructive Surgery
Textbook
Published Author
Contributions to the academic literature of facial plastic surgery
Dual board certification in both Facial Plastic & Reconstructive Surgery and Otolaryngology — Head & Neck Surgery.
01 · Why Dr. Mourad
Diagnosis first, then a plan that fits.
Dr. Mourad approaches male buccal fat removal with deliberate restraint — the difference between an athletic-looking jawline and a hollow one is millimetres.
Patients are screened for natural mid-face fat distribution and projected facial aging trajectory.
When fuller jawline definition is the goal, jawline augmentation or chin work is often a better — and more reversible — first step than fat removal.
02 · Ideal Candidates
Who benefits most from this operation.
Candidacy is determined together at consultation. The most satisfied patients share three things in common.
I
Full Lower Cheeks
Men with persistent lower-cheek fullness disproportionate to the rest of the face that does not change with body composition.
II
Mature Facial Structure
Generally late twenties or older, with stable adult facial proportions.
III
Conservative Goals
Men seeking subtle refinement of the lower cheek — never aggressive hollowing.
Before & After
Real results, real patients.
Every case is unique — tailored to individual anatomy and goals. Browse representative outcomes from the Manhattan practice.
If this describes you, the next step is a quiet, unhurried conversation — not a sales call.
An Honest Note
When this operation may not be right for you.
Men under 25 with naturally thin mid-face fat — the procedure will age poorly.
Men seeking dramatic transformation are typically better served by chin or jawline augmentation.
Men whose dissatisfaction is rooted in body-image concerns benefit from a longer evaluation before any irreversible facial procedure.
Men who have lost significant weight recently should wait until weight is stable before considering removal.
03 · Approaches
Three paths to a defined lower face.
Male buccal fat removal is a conservative operation. The right plan depends on whether the goal is isolated cheek refinement or part of a broader jawline restructuring.
1 of 3 · Conservative Buccal Reduction
04 · Technique
Conservative vs combined approach.
Two paths through the same starting concern. The right choice depends on whether the issue is the cheek itself or the overall lower-face balance.
Buccal Only
Partial reduction in the right patient
When the lower cheek fullness is the isolated concern and the chin and jawline are already well-balanced, a measured partial reduction is the right operation.
The change is modest and predictable. Over-reduction is avoided as a matter of principle.
Combined
Chin or jawline augmentation paired
When the lower face would benefit more from added definition than from subtracted volume, a chin or jawline implant — sometimes paired with very conservative buccal reduction — produces a better-balanced result.
This is, in many male patients, the right answer to a question that was framed as "less" but is really about "more structure."
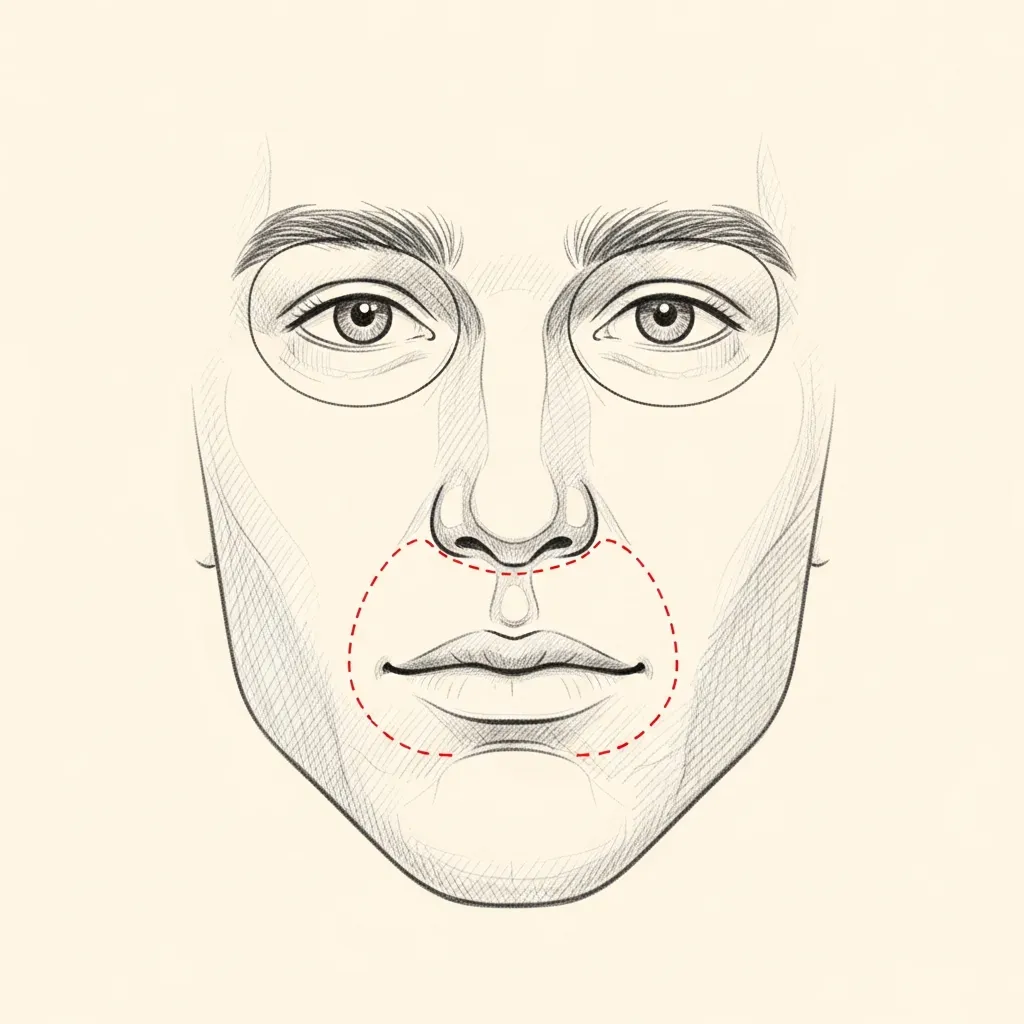
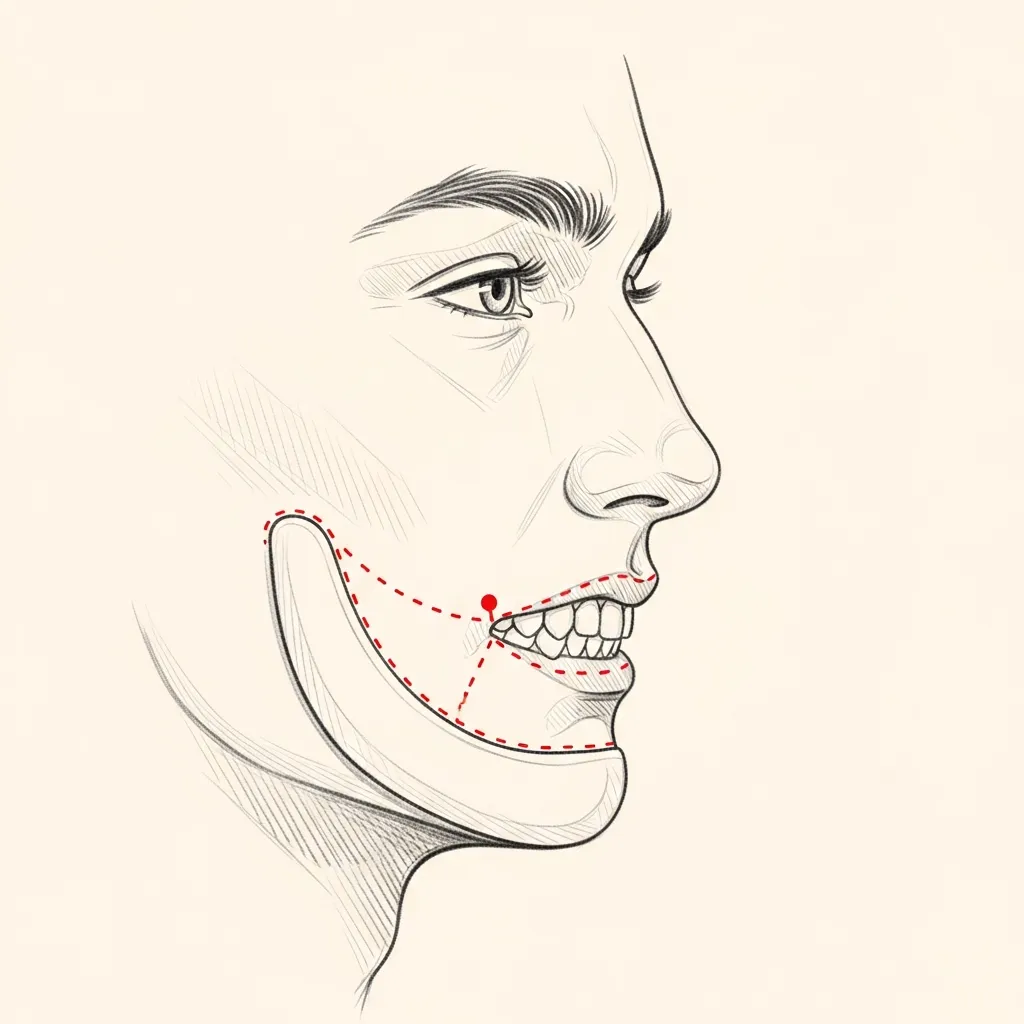
Illustrative diagrams. The right plan is determined together based on overall facial balance.
Begin the conversation
A careful, honest evaluation is the right first step.
Cost, Financing & Insurance
Male Buccal Fat Removal Cost, Financing & Insurance in NYC
The cost of male buccal fat removal depends on the surgical plan, whether it is combined with other facial contouring, the type of anesthesia, and the surgical setting. Candidacy is evaluated carefully to maintain natural masculine facial proportions.
Buccal fat removal is a cosmetic procedure and is typically self-pay. After consultation, our office provides a personalized estimate based on the recommended plan. Financing may be available for qualified patients through third-party healthcare financing providers.
What May Affect Cost
- Whether performed alone or combined
- Facial anatomy and goals
- Type of anesthesia
- Surgical setting
- Postoperative care
- Maintaining masculine proportions
This information is educational and is not a guarantee of pricing, insurance coverage, reimbursement, financing approval, or surgical candidacy. A personalized estimate is provided after consultation. Insurance coverage depends on the patient’s plan, medical necessity, documentation, and carrier requirements. Financing terms are determined by third-party financing providers.
06 · Recovery
What healing actually looks like.
Stage 01
First 24 Hours
Initial recovery focuses on rest, hydration, and following all post-operative instructions exactly. Pain is managed with multi-modal non-narcotic protocols where appropriate.
Stage 02
Week 1
Swelling and bruising peak in the first few days and improve steadily through the first week. Most patients are presentable for casual social activity by the end of week two.
Stage 03
Weeks 2 – 4
Through weeks two to four the early result begins to settle. Light cardio resumes around three weeks; vigorous exertion and contact activities are deferred per the operative plan.
Stage 04
Months 1 – 6
The final refined result emerges progressively over the following months as residual swelling continues to resolve. Follow-up visits are scheduled across the first year.
Have a specific question?
Send a brief note describing your anatomy or concerns — the office will route it directly to Dr. Mourad for review.

Before You Arrive
Your consultation, prepared.
Bring photographs relevant to your concern, when available.
Bring records from any prior surgery, when available.
List current medications, supplements, and blood-thinning agents.
Note any prior anesthesia issues or chronic medical conditions.
Allow 60 minutes for the first consultation.
Bring questions; no decisions are made at the first visit.
Frequently Asked
Patient questions, honestly answered.
The buccal fat pad is a discrete deep cheek compartment adjacent to the buccinator muscle. In men, its volume influences how the cheek projects against the jaw and chin. The pad has lobes and extensions that determine surface contour changes after excision. Clinical examination and standardized photos help distinguish pad prominence from superficial fat. An in‑person consultation is required to determine if excision is appropriate.
Good candidates have persistent, localized mid‑cheek fullness that does not change with weight. Candidates should have sufficient bone projection and skin quality to support a leaner cheek. Patients with thin facial types or a family history of facial lipoatrophy may be poor candidates. Adjunctive skeletal or volumizing options are considered when needed. An in‑person visit is required to confirm candidacy and plan safely.
Most procedures use an intraoral mucosal incision to avoid external scars. Under monitored anesthesia care or general anesthesia, the surgeon gently teases the buccal fat pad into view and performs a conservative excision with careful hemostasis before closing. The operation alone commonly takes 30–60 minutes. The anesthesia plan and exact technique are finalized during the consultation.
Short‑term risks include bleeding, intraoral wound issues, temporary numbness, and localized infection. Long‑term risks include over‑resection and progressive midface hollowing as aging alters soft tissue and bone. Predicting late hollowing is imperfect; a conservative preservation strategy and combined planning reduce risk. Individual risk and mitigation are discussed in detail at an in‑person consultation.
Most men experience modest swelling and bruising for about 3–10 days. Many return to desk work in 3–7 days. Strenuous activity and heavy lifting are typically restricted for 2–3 weeks. Oral hygiene and a soft diet are usually advised for the first 5–10 days. A personalized recovery timeline is provided in clinic.
An intraoral approach avoids external skin scars because the incision is inside the mouth. Injury to the facial nerve is rare when the correct plane is followed, and major motor branches are not in the operative field. Temporary numbness or altered sensation near the incision can occur and typically resolves. Functional and aesthetic risks are reviewed during an in‑person consultation.
Yes. Combining buccal fat removal with chin or jaw augmentation often improves facial balance and reduces the chance of an isolated hollowed appearance. Options include chin implants, sliding genioplasty, or targeted filler based on skeletal needs. Combined procedures change operative time and recovery and are planned case‑by‑case. A face‑to‑face visit is necessary to determine the optimal combination.
Once buccal fat is excised it cannot be replaced directly, but restorative options exist. Correction options include autologous fat grafting, deep cheek fillers, or structural augmentation such as cheek implants. Timing varies; many surgeons wait 12–24 months to assess natural changes before elective restoration. An in‑person evaluation is required to plan the appropriate restorative approach.
Buccal fat is a distinct pad deep to the cheek muscles; superficial facial fat sits in the subcutaneous layer and changes more with weight. Weight loss typically reduces superficial fullness more than the buccal pad. Palpation and photographic analysis help separate localized pad prominence from diffuse adiposity. An in‑person exam determines whether surgery or non‑surgical options suit you best.
The consultation includes focused history, physical exam, and standardized photography emphasizing bone projection and soft‑tissue depth. Dr. Mourad discusses conservative excision volumes, preservation priorities, and potential adjunctive procedures with realistic recovery ranges. Candidate suitability, complication risks, and revision pathways are reviewed to support shared decision‑making. A face‑to‑face visit is required to finalize any surgical recommendation.
Explore Further
Related procedures & resources
Cheek contouring is evaluated alongside the jawline and the wider face. These pages explain the related options.
Buccal Fat Removal
The core procedure and its candidacy considerations.
Read moreChin Augmentation
Improving chin projection can balance the lower-face profile.
Read moreFacelift
For patients whose primary concern is lower-face descent rather than fullness.
Read moreBefore & After Gallery
Representative facial contouring cases, photographed with written consent on file.
Read moreRequest a Consultation
Begin with an unhurried clinical evaluation.
Read moreThe Most Important Step
Your expert consultation.
A careful evaluation by a double board-certified physician is the right first step. The conversation is unhurried, the diagnosis is honest, and the operative plan is built around what your anatomy can sustain and what you actually want.