Double Board Certified · Reconstructive Rhinoplasty
Saddle Nose Deformity — structural collapse with a structural answer.
Saddle nose deformity is a collapse of the dorsum — the bridge of the nose — that produces a characteristic concave profile. The cause may be prior trauma,…
ABFPRS
Facial Plastic & Reconstructive Surgery
ABOto
Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
In Consultation
"A saddle deformity is rebuilt with structure — cartilage, structural support, and a careful plan that respects what tissue remains."
A Note from Dr. Mourad
"Saddle nose deformity is a collapse of the dorsum — the bridge of the nose — that produces a characteristic concave profile. The cause may be prior trauma, prior surgery, systemic disease, or chronic inflammatory process; the reconstructive plan is always structural."
— Dr. Moustafa Mourad, MD
Overview
What is saddle nose deformity?
Saddle nose deformity is a structural collapse of the dorsum (bridge) of the nose, in which loss of cartilaginous support produces a depressed middle vault, an over-rotated tip, and a shortened nasal length. The depressed contour gives the bridge the appearance of a saddle.
Causes include prior septal surgery with over-resection of the L-strut, trauma with disruption of dorsal support, granulomatous diseases such as granulomatosis with polyangiitis, drug-induced cartilage loss (notably cocaine), and longstanding septal perforation with dorsal collapse. Identifying the cause matters for both treatment and long-term care.
Reconstruction is structural and typically requires significant cartilage grafting — most often from the rib — to rebuild dorsal support and restore the length of the nose. It is one of the more demanding operations in revision rhinoplasty and is staged according to the underlying cause.
An Established Academic Authority
Double board certification. Fellowship director. Published author. A surgeon's surgeon.
ABFPRS
Board Certified
American Board of Facial Plastic & Reconstructive Surgery
ABOto
Board Certified
American Board of Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
American Academy of Facial Plastic and Reconstructive Surgery
Textbook
Published Author
Contributions to the academic literature of facial plastic surgery
Dual board certification in both Facial Plastic & Reconstructive Surgery and Otolaryngology — Head & Neck Surgery.
Castle Connolly Top Doctor — Plastic Surgery, 202602 · Symptoms
How this condition typically presents.
Three patterns are most common. Patients often recognise themselves in one or more of these.
I
Concave Dorsal Profile
A visibly depressed dorsum on lateral profile, often described as a saddle or scoop.
II
Nasal Obstruction
Collapse of the dorsal septum frequently reduces the internal nasal valve and impairs breathing.
III
Tip Drop & Loss of Projection
Loss of dorsal support often causes the tip to rotate downward and lose projection.
03 · Anatomy
Cartilage & structural support.
Saddle reconstruction is, fundamentally, a cartilage operation. The donor site is chosen by the volume of structure required.
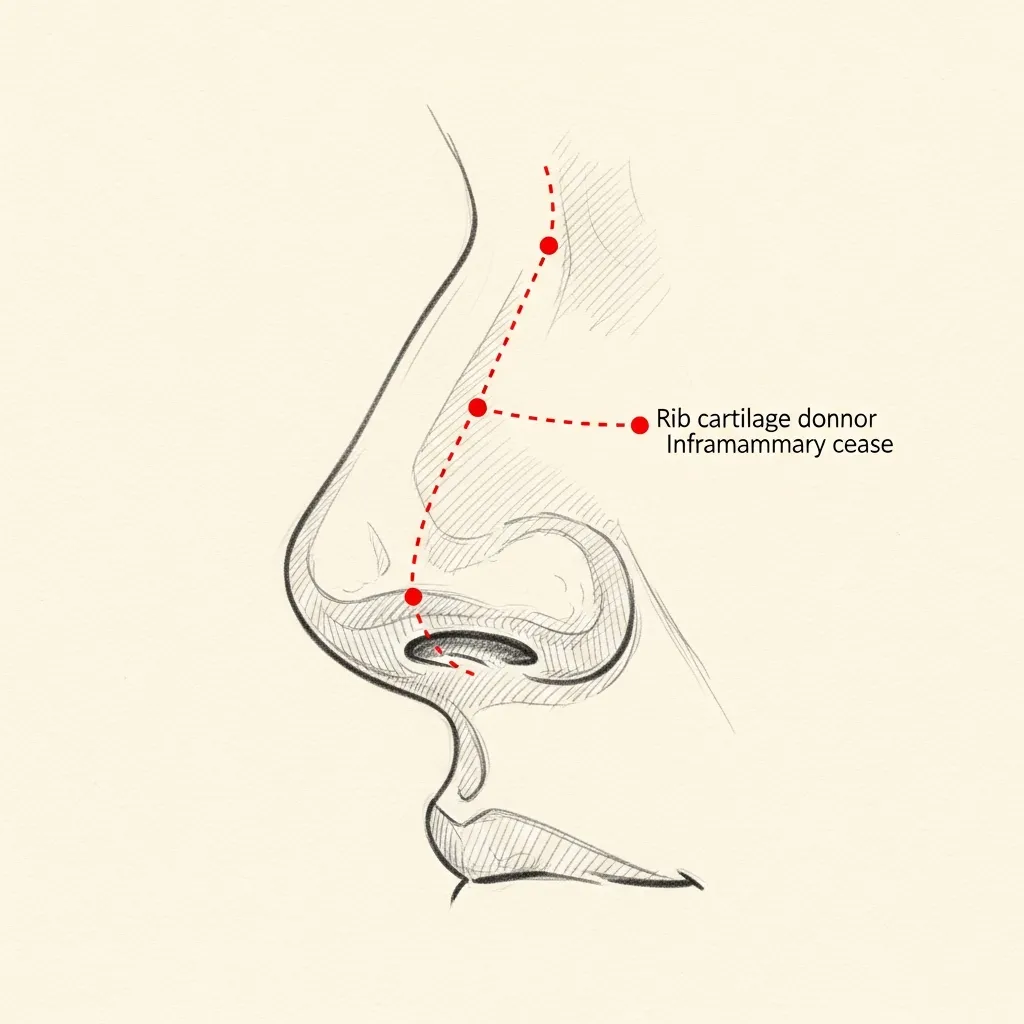
Costal
Rib cartilage for significant reconstruction
Costal (rib) cartilage is the workhorse of significant saddle reconstruction — providing abundant, strong, sculptable material when septal and auricular sources are inadequate.
Harvest is performed through a small hidden incision in the natural inframammary crease, with multimodal non-narcotic pain management.
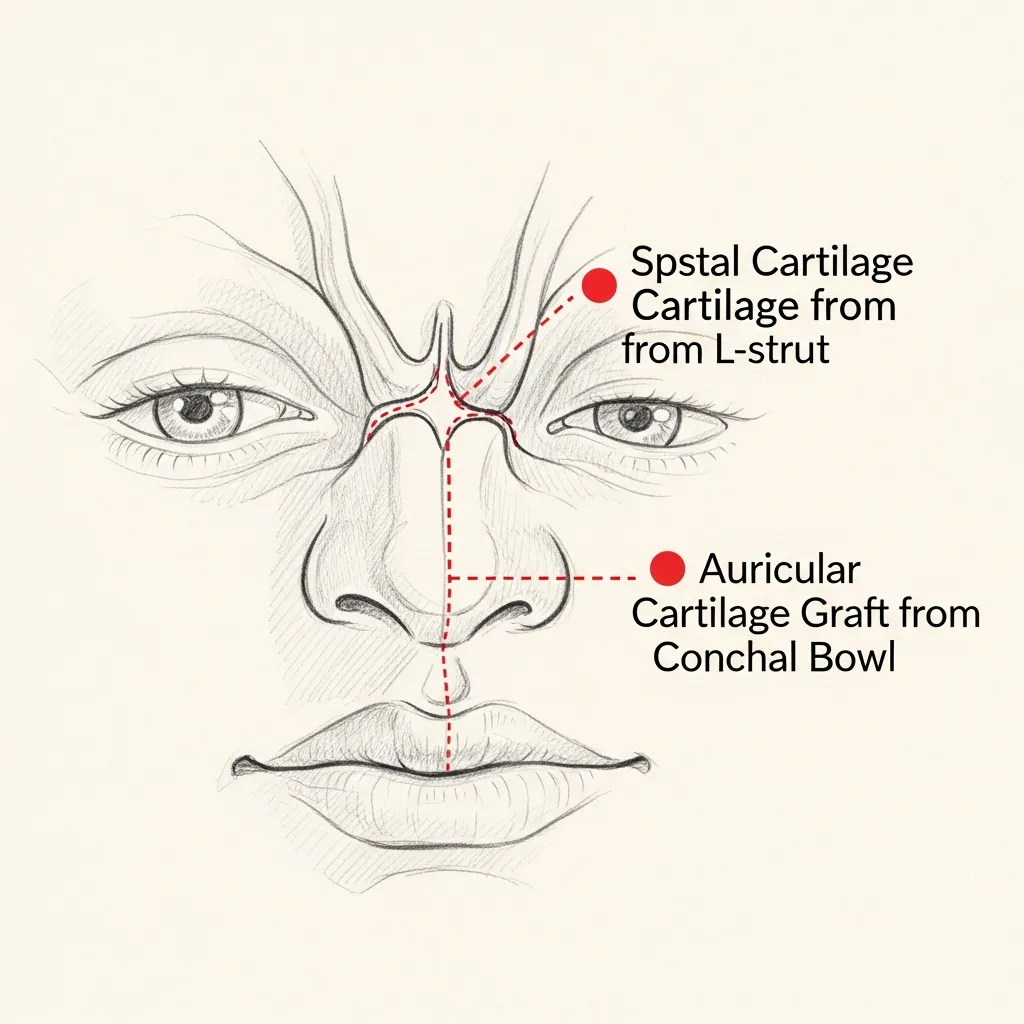
Septal & Ear
When local supply is sufficient
For smaller saddle defects, residual septal cartilage and auricular cartilage from behind the ear may provide enough structural support — sparing the patient a rib harvest.
The choice is made case-by-case based on the volume of correction needed and what remains available.
Illustrative diagrams. The reconstructive plan is determined by the underlying cause and the volume of structural loss.
04 · Diagnosis
How the diagnosis is made.
Diagnosis is clinical and supplemented by imaging when relevant — particularly to assess the bony framework and identify any underlying inflammatory process.
The cause is identified — prior trauma, prior surgery, granulomatous disease, vasculitis, or chronic intranasal drug use — because reconstruction will not hold if the underlying process is still active.
Photographs from before the deformity developed, when available, guide the reconstructive target.
05 · Treatment Options
Treatments matched to the diagnosis.
Treatment is individual. The right answer ranges from optimised medical therapy to a focused procedure to definitive surgery.
Cartilage Reconstruction
Structural cartilage grafting — septal, auricular, or costal — to rebuild the collapsed dorsum.
Learn More
Revision Rhinoplasty
When the deformity is post-surgical, full structural revision is the right operation.
Learn More
Septal Perforation Repair
Often combined with saddle nose repair when a perforation is part of the structural loss.
Learn More
01 · Why Dr. Mourad
Diagnosis first, treatment second.
Dr. Mourad specialises in reconstructive and revision rhinoplasty and approaches saddle deformity with deliberate structural planning — the goal is durable correction, not a temporary fix.
The underlying cause is identified and addressed first; if active inflammatory disease is present, control is achieved before reconstruction is attempted.
Cartilage source is chosen based on the volume of structural support required — most commonly costal cartilage for significant collapse.
When to Seek Care
When to seek care promptly.
New onset of nasal collapse after trauma — evaluate within days.
Rapid worsening of nasal shape in the setting of known systemic disease — evaluate promptly.
Signs of infection or wound problems after recent surgery — evaluate urgently.
Bloody nasal discharge that does not resolve — evaluate within days.
Outlook
What to expect.
When the diagnosis is correct and the right treatment is applied, the outlook is generally good. Most patients describe meaningful improvement in symptoms and day-to-day function.
When symptoms persist despite treatment, the workup is re-opened. Persistent symptoms with no answer almost always mean the diagnosis is incomplete.

Living Well
Day-to-day measures that help.
Daily saline irrigation, control of indoor allergens, and good sleep hygiene meaningfully reduce day-to-day symptoms for many patients.
Medical therapy, when prescribed, works best when used consistently rather than as needed — this is one of the most common reasons treatment seems to fail.
Frequently Asked
Patient questions, honestly answered.
A saddle nose deformity is loss of dorsal height from failure of the septal support column or middle vault. Causes include excessive septal cartilage removal during prior surgery, untreated septal hematoma after trauma, focal infection, or inflammatory tissue loss. The deformity frequently alters tip position and can narrow the internal nasal valve, producing obstructive symptoms. Definitive evaluation combines history, focused exam, nasal endoscopy, and targeted imaging to identify the mechanism before reconstruction.
Start by establishing a timeline: note when contour change and symptoms began relative to any surgery or injury. Prior operative reports, intraoperative photos, and records of postoperative complications, like hematoma or infection, are especially informative. Nasal endoscopy and non-contrast CT can show residual septal cartilage, scarring, mucosal disease, or bony injury that point to a cause. Final determination requires an in-person assessment synthesizing history, exam, and imaging.
Restoring dorsal and septal support often improves the internal nasal valve and nasal airflow, but improvement is not guaranteed in every patient. Airway outcome depends on collapse severity, concurrent problems such as turbinate hypertrophy or external valve collapse, and the reconstructive plan chosen. Reconstruction commonly pairs dorsal support (spreader grafts or dorsal onlay) with valve-specific procedures when indicated. A preoperative assessment clarifies realistic airway goals and whether staged or combined interventions are required.
A focused workup usually includes nasal endoscopy to assess mucosal health, perforation, and scarring, plus non-contrast CT when structural detail is required. CT helps define septal loss, bony dorsum status, and prior fracture patterns that affect graft planning. Laboratory testing or rheumatology evaluation is indicated if an inflammatory, infectious, or vasculitic process is suspected. Final testing is individualized after the consultation.
Common donor sites are septal cartilage, auricular cartilage, and costal (rib) cartilage; each has trade-offs in strength, availability, and donor-site morbidity. Septal cartilage is preferred when adequate local tissue remains. Auricular cartilage is useful for contouring smaller defects but offers limited load-bearing capacity. Costal cartilage provides robust structural support for large central defects or when local cartilage is depleted, though it requires a chest incision and separate donor-site recovery.
Rib cartilage is considered when septal tissue is insufficient or absent, or when a central, load-bearing column is required to restore dorsal height. Large central dorsum deficits, previous extensive septal resection, or multiple prior rhinoplasties commonly necessitate costal grafts. The decision also weighs patient factors such as donor-site tolerance and prior chest surgery. Final graft choice is made after in-person exam and review of prior imaging and operative records.
Candidates typically have documented structural loss on exam or imaging, symptomatic internal valve compromise, or persistent contour deformity after conservative care. Patients with functional complaints (obstruction) or combined cosmetic and airway goals are commonly appropriate for surgery. Those with isolated aesthetic concern may still be referred for evaluation; candidacy depends on anatomy and realistic expectations. Final candidacy is determined in clinic after a full history, exam, and review of prior records or imaging.
Relative contraindications include active systemic vasculitis or uncontrolled inflammatory disease, ongoing intranasal substance use, active infection, and poor wound-healing risk from uncontrolled diabetes or heavy smoking. Severe cardiopulmonary disease or inability to tolerate anesthesia also preclude elective reconstruction. Optimization steps include disease control with the treating specialist and smoking cessation, typically for at least 4–8 weeks preoperatively when feasible. Timing for surgery after disease control is individualized and generally requires medical clearance.
Immediate postoperative days 0–7: nasal splints or soft dressings are common; patients usually have mild-to-moderate pain controlled with oral medication and should limit activity. Weeks 1–2: external splints and sutures are often removed around day 7–10; most patients return to desk work within 1–2 weeks. Weeks 3–6: bruising resolves and nasal breathing typically improves; avoid heavy lifting and contact sports for 6–8 weeks. Weeks 7–12: most routine activities resume; dorsal contour continues settling. Months 3–6: graft integration progresses and swelling declines substantially. Months 6–12: final contour and airway result continue to refine, with most changes complete by 12 months. Rib donor-site soreness commonly improves over 2–6 weeks, though full chest-strength recovery may take longer.
Risks include graft warping or partial resorption, persistent or recurrent collapse, infection, septal perforation, and persistent airway obstruction or contour asymmetry. Donor-site complications for rib harvest include pain, contour irregularity, or scarring. Revision reconstruction carries greater technical complexity due to scarring and altered planes. Potential risks are reviewed in detail during consultation and balanced against expected benefits.
Staged reconstruction is sometimes necessary when mucosal health is uncertain or when an underlying disease requires control before definitive grafting. A staged approach can allow mucosal healing or medical therapy to take effect and reduce the risk of graft failure. Typical intervals between stages are commonly 3–6 months but are individualized based on healing and disease stability. The timing and need for staging are decided collaboratively with any medical specialists involved.
Bring all prior operative reports, intraoperative photos if available, and any prior imaging such as CT scans to the visit. Prepare a concise timeline of symptoms, surgeries, trauma, intranasal medications or substances, and systemic illnesses. Expect focused nasal exam, possible bedside endoscopy, and a discussion of graft options and staged planning if needed. If inflammatory disease is suspected, bring relevant specialist notes or lab results for coordinated planning.
The Most Important Step
Get an expert evaluation.
A careful evaluation by a double board-certified physician is the right first step. The conversation is unhurried, the diagnosis is honest, and treatment is matched to what you actually have.