Double Board Certified · Functional Nasal Surgery
Septoplasty in NYC — a quiet operation that returns the breath.
Septoplasty is one of the most rewarding operations in functional nasal surgery. The change is internal — the architecture of the airway is rebuilt — but the impact on sleep, exercise, and daily energy is often profound.
ABFPRS
Facial Plastic & Reconstructive Surgery
ABOto
Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
In Consultation
"Most patients tell me they did not realise how restricted their breathing had been until it was corrected."

A Note from Dr. Mourad
"Septoplasty is one of the most rewarding operations in functional nasal surgery. The change is internal — the architecture of the airway is rebuilt — but the impact on sleep, exercise, and daily energy is often profound."
— Dr. Moustafa Mourad, MD
Medically reviewed by Moustafa Mourad, MD, FACS — dual board-certified Facial Plastic & Reconstructive Surgeon and Otolaryngologist (Head & Neck Surgery).
Last reviewed: June 2026
Is this the right page for you?
This page is for
- Your main problem is breathing — persistent blockage on one or both sides, often worse at night or with exercise.
- A deviated septum has been identified as the cause of your nasal obstruction.
- You want to improve the airway without changing how your nose looks.
You may be looking for
- If you also want to change the appearance of your nose, see septorhinoplasty.
- If collapse of the nasal sidewall on breathing in is the issue, see nasal valve collapse treatment.
Overview
What is septoplasty?
Septoplasty is a functional surgical procedure that straightens the nasal septum — the wall of cartilage and bone that divides the two nasal passages. The operation is performed entirely through the nostrils, with no external incisions, and removes or repositions the deviated portion while preserving structural support for the nose.
It is considered when a deviated septum produces nasal obstruction, recurrent infections, post-nasal drip, sleep disruption, or recurrent nosebleeds that have not responded to medical therapy. Diagnosis is made on examination, often supported by nasal endoscopy and, when indicated, imaging.
Septoplasty is a purely functional operation. When the external shape of the nose is also a concern, septoplasty can be combined with rhinoplasty (septorhinoplasty) so both problems are addressed in a single recovery rather than across two operations.
An Established Academic Authority
Double board certification. Fellowship director. Published author. A surgeon's surgeon.
ABFPRS
Board Certified
American Board of Facial Plastic & Reconstructive Surgery
ABOto
Board Certified
American Board of Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
American Academy of Facial Plastic and Reconstructive Surgery
Textbook
Published Author
Contributions to the academic literature of facial plastic surgery
Dual board certification in both Facial Plastic & Reconstructive Surgery and Otolaryngology — a combination held by a small number of physicians nationally.
02 · Ideal Candidates
Who benefits most from this operation.
Candidacy is determined together at consultation. The most satisfied patients share three things in common.
I
Persistent Nasal Obstruction
One- or two-sided difficulty breathing through the nose that does not resolve with medical therapy — sprays, irrigations, or allergy treatment.
II
Sleep & Exercise Impact
Mouth breathing at night, snoring, dry mouth on waking, or a clear reduction in aerobic capacity that traces to the airway, not the lungs or heart.
III
Documented Deviation
A deviated septum confirmed on examination — and frequently on imaging — that is the structural cause of the obstruction, not allergic mucosal swelling alone.
If this describes you, the next step is a quiet, unhurried conversation — not a sales call.
An Honest Note
When this operation may not be right for you.
If your symptoms are driven primarily by allergies or chronic rhinitis, medical therapy or turbinate-directed treatment may resolve the issue without operating on the septum.
Active inflammatory sinus disease is treated first; septoplasty is rarely performed on an infected airway.
Smokers and patients on certain blood thinners require a planned medical optimization window before any nasal surgery.
Cosmetic complaints about the external nose are not addressed by a septoplasty alone — that conversation belongs to rhinoplasty or septorhinoplasty.
03 · Approaches
The full range of options.
Septoplasty is rarely a stand-alone operation. The right plan considers companion procedures — turbinate, valve, sinus — and accounts for whether prior surgery has already shaped the anatomy.
1 of 6 · Standard Septoplasty
04 · Technique
Endoscopic vs open septoplasty.
Most modern septoplasties are performed entirely through the nostrils with endoscopic visualization. An open approach is reserved for the small subset of patients whose anatomy requires it.
Endoscopic
Endonasal
An incision is made inside the nostril, and the deviated portions of the cartilage and bone are conservatively removed or repositioned. The mucosal lining is preserved on both sides of the septum.
There are no external scars. Recovery is straightforward, and the airway change is typically appreciated as swelling resolves over the following weeks.
Open
Septorhinoplasty Access
When the septum is severely deviated, especially in revision cases, an open approach through a small columellar incision provides the exposure required to rebuild the septum with cartilage grafts.
This is the standard approach when functional septoplasty is being performed alongside cosmetic rhinoplasty as a single operation.
Illustrative diagrams. The appropriate approach is determined individually at consultation.
01 · Why Dr. Mourad
A surgeon trusted by surgeons for this operation.
Dr. Moustafa Mourad is double board-certified by the American Board of Facial Plastic & Reconstructive Surgery and the American Board of Otolaryngology — Head & Neck Surgery, and serves as an AAFPRS Fellowship Director.
The practice concentrates on the operations of the face, nose, and sinuses — and on the patients other surgeons have found challenging.
Every consultation is unhurried, every plan is individual, and no operation is recommended unless it is the right one.
Begin the conversation
Functional nasal evaluation. A real conversation about your breathing.
Cost, Financing & Insurance
Septoplasty Cost, Financing & Insurance in NYC
Septoplasty cost depends on the complexity of the septal deviation, whether turbinate reduction is performed at the same time, the type of anesthesia, and the surgical facility. Each plan is individualized after a nasal airway evaluation.
Because septoplasty is a functional procedure that treats nasal obstruction, it may be covered by insurance when it is medically necessary. Coverage often depends on symptoms, examination findings, prior medical treatment, and the requirements of the patient’s insurance plan. Our office can help review benefits and guide patients through preauthorization when appropriate.
What May Affect Cost
- Severity of septal deviation
- Whether turbinate reduction is included
- Type of anesthesia
- Surgical facility
- Prior nasal surgery
- Insurance plan requirements
This information is educational and is not a guarantee of pricing, insurance coverage, reimbursement, financing approval, or surgical candidacy. A personalized estimate is provided after consultation. Insurance coverage depends on the patient’s plan, medical necessity, documentation, and carrier requirements. Financing terms are determined by third-party financing providers.
05 · In Dr. Mourad's Words
Educational videos.
Short educational films and patient perspectives from the Manhattan practice.
Dr. Mourad in Practice
An overview of the practice and philosophy.
Patient Perspective
A patient discusses her experience before, during, and after surgery.
Inside the Consultation
How Dr. Mourad evaluates anatomy, goals, and candidacy.
Anatomy · Illustrated
What septoplasty corrects, seen from below.
These anatomical drawings are illustrative, not patient photographs. The first shows a deviated septum buckled to one side, restricting airflow through one nostril. The second shows the same view after septoplasty, with the septum straightened and airflow restored through both sides.
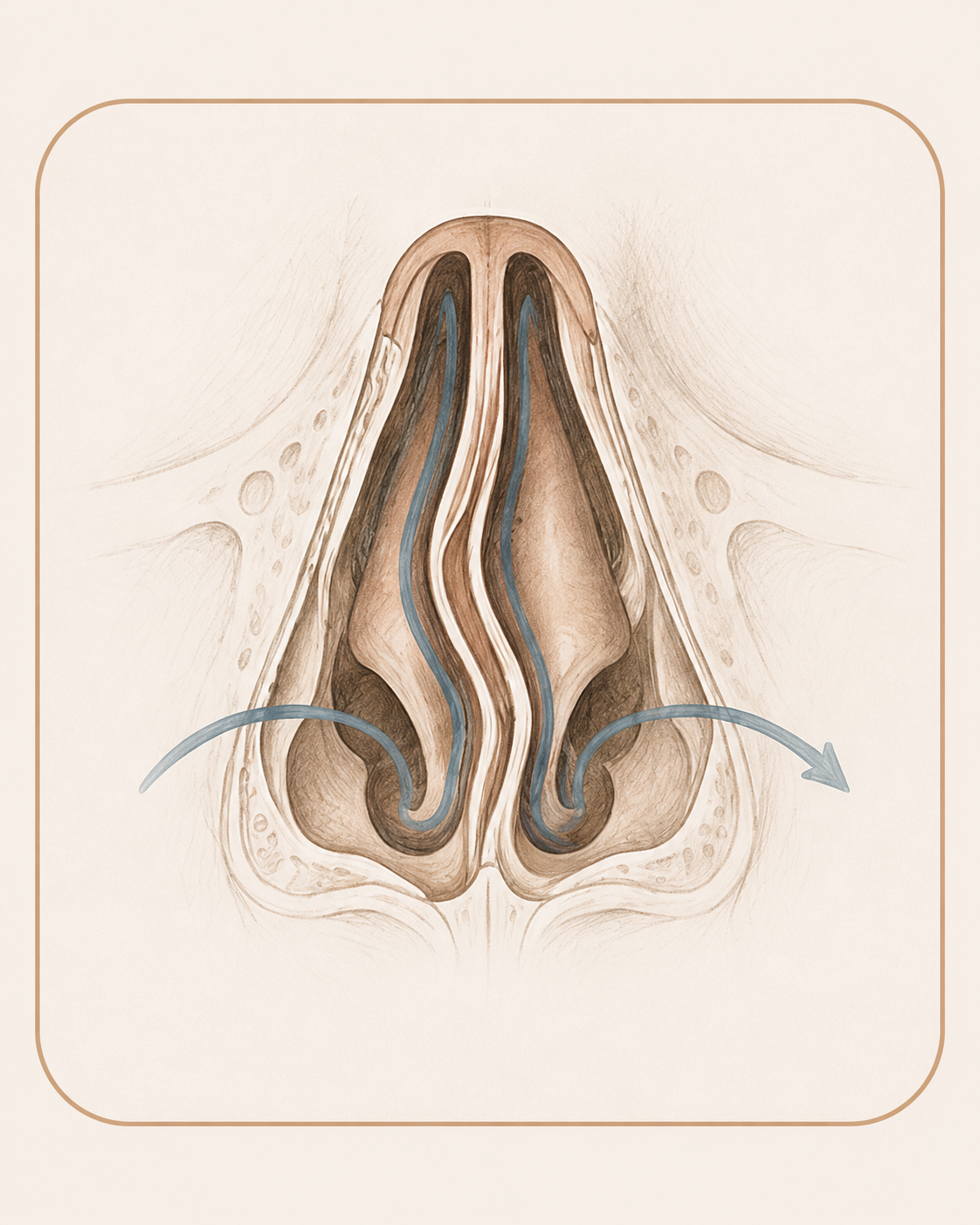
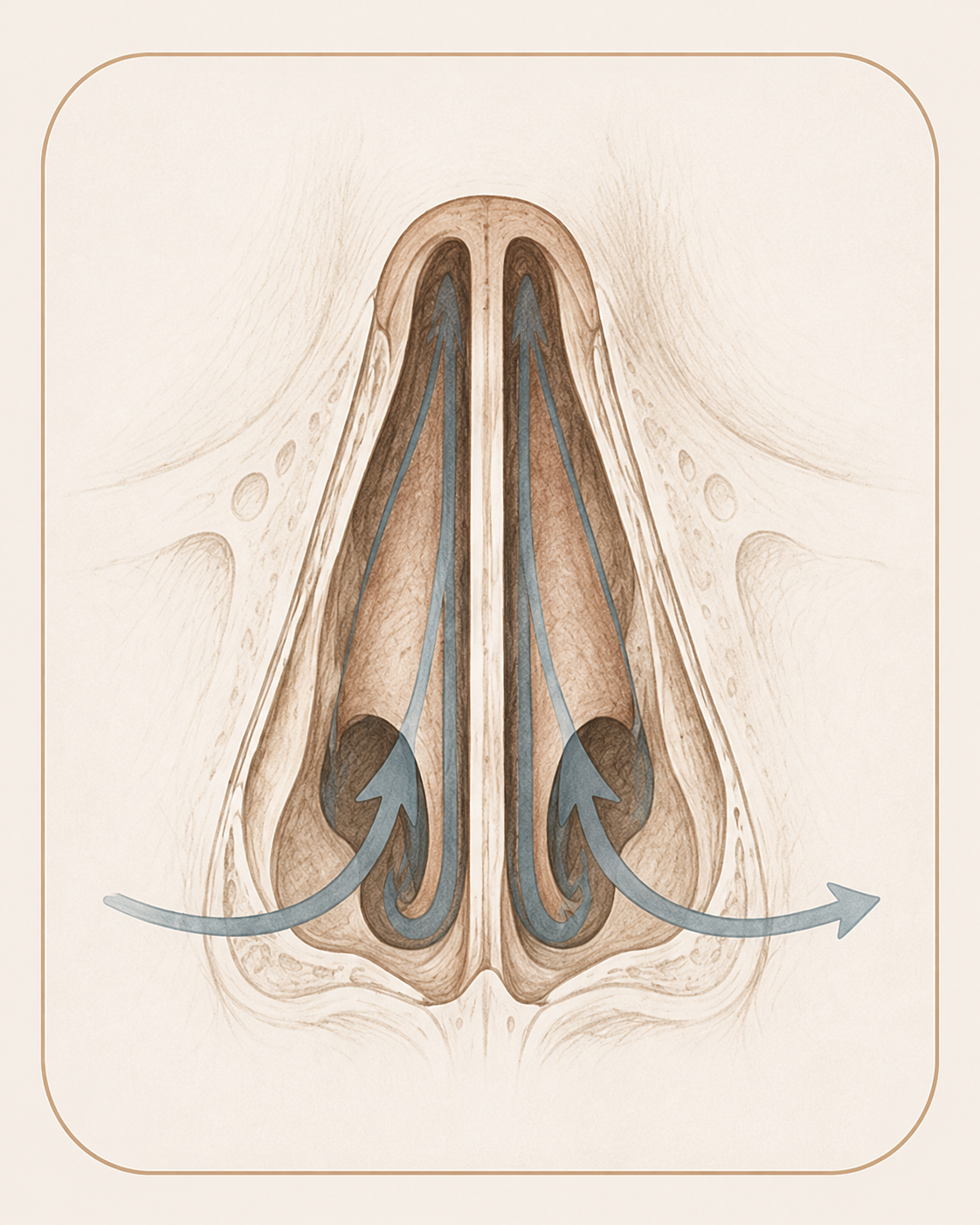
Basal anatomical view · Illustrative diagram · Not to scale
06 · Recovery
What healing actually looks like.
Stage 01
First 24 Hours
Internal splints, when used, are removed at the first post-operative visit around day seven. There is no external dressing. Mild congestion is expected as the lining heals.
Stage 02
Week 1
Through the first week, light activity is encouraged. Heavy lifting and exercise are deferred. Most patients return to office work within a few days.
Stage 03
Weeks 2 – 4
Through weeks two to four, congestion progressively clears. Saline irrigation is continued. The airway improvement becomes increasingly evident.
Stage 04
Months 1 – 12
From one month onward, scar tissue settles and the final airway is appreciated. Long-term, the corrected septum is stable.
Have a specific question?
Send a brief note describing your anatomy or concerns — the office will route it directly to Dr. Mourad for review.

Before You Arrive
Your consultation, prepared.
Bring any prior CT scans of the nose or sinuses if available.
Note any prior nasal surgery, trauma, or septal injuries.
List allergy medications, decongestants, and nasal sprays you currently use.
Stop blood-thinning medications and supplements per the timeline you will receive.
Allow 60 minutes for a focused functional nasal examination.
No surgical decisions are made at the first visit — that is intentional.
Patient Reviews
Septoplasty and Breathing Patient Experiences
Selected public patient reviews. Individual experiences vary.
“I can now say I can breathe better than I ever have”
Real patient experiences
Selected public reviews from patients of the practice.
Your privacy matters
We never share personal health information.
Board-certified expertise
Dual board-certified facial plastic and reconstructive surgeon.
Individual results vary. Reviews reflect individual experiences and are not a guarantee of outcome.
Frequently Asked
Patient questions, honestly answered.
Many patients notice partial improvement within days as packing or crusting resolves. Meaningful airway change usually evolves over 2–6 weeks as mucosal swelling subsides. Healing and functional refinement can continue for three to six months. Individual timelines vary and are reviewed during follow‑up visits.
Pure septoplasty corrects internal septal alignment and is not intended to alter external nasal shape. Minor contour changes can occur if septal support is modified, but planned cosmetic changes require septorhinoplasty. If you want both airway and aesthetic modification, we discuss combined septorhinoplasty during consultation.
Most patients resume desk work in 3–7 days if comfortable and without significant bleeding. Strenuous exercise and heavy lifting are usually restricted for 3–6 weeks. Flying is often safe after initial crusting or packing resolves, commonly after 1–2 weeks, but check with your surgeon for individual guidance. Concurrent procedures can lengthen recovery.
Office evaluation includes external inspection, nasal valve assessment, and nasal endoscopy to document anatomy. Photographic and endoscopic images are used for planning and insurance documentation. CT imaging is reserved for complex deformity, prior surgery, or concurrent sinus disease. Findings guide whether turbinate or valve procedures are added to septoplasty.
Septoplasty focuses on internal septal alignment to improve airflow. Septorhinoplasty combines septal correction with external nasal contouring when aesthetic change is desired. Turbinate reduction addresses mucosal or bony enlargement that narrows the airway and is commonly combined with septoplasty. The surgical plan is individualized based on functional and cosmetic goals.
Persistent obstruction often reflects unrecognized nasal valve collapse, residual turbinate hypertrophy, or incomplete cartilage correction. Scar tissue from prior surgery can also limit airway gain. Revision requires careful endoscopic reassessment and may include grafting, valve stabilization, or turbinate procedures. Revision planning is bespoke because altered anatomy and scarring change technique and recovery.
Insurance coverage varies by plan and typically requires documentation of functional impairment and prior conservative therapy. Useful documentation includes exam notes, endoscopic images, and records of medical therapy such as topical steroids. Preauthorization is commonly required and our office assists with paperwork, but final coverage decisions rest with the insurer. Patients should check benefits before scheduling.
Revision septoplasty often needs more extensive dissection, scar release, and structural grafting because native support may be altered. Cartilage grafts or staged reconstruction can be required to restore framework and prevent collapse. Operative time and complexity are generally greater than for a primary septoplasty. Outcomes can be improved with meticulous planning but recovery and risks may be higher.
Mild to moderate congestion and facial pressure are common; severe pain is uncommon. Analgesia usually consists of acetaminophen and selective short opioid prescriptions for breakthrough pain when needed. Light anterior bleeding or posterior drainage can occur for 48–72 hours; persistent heavy bleeding is uncommon and should prompt contact with the surgeon. Head elevation and avoidance of straining help reduce bleeding.
Yes. Topical nasal corticosteroids, antihistamines, and targeted allergy care should be optimized when appropriate. For some patients with dynamic collapse, external nasal valve devices can offer temporary benefit. When structural deviation continues to limit airflow after adequate conservative care, septoplasty is considered. Final decisions follow objective assessment and shared decision‑making.
Clinical references
This page draws on published clinical practice guidelines and public-health references. These sources inform general patient education and do not replace an individual evaluation with Dr. Mourad.
- 01American Academy of Otolaryngology–Head and Neck Surgery Foundation. Clinical Consensus Statement: Septoplasty with or without Inferior Turbinate Reduction. Otolaryngology–Head and Neck Surgery. 2015;153(5):708–720. AAO-HNSF consensus
- 02U.S. National Library of Medicine (MedlinePlus). Nose Injuries and Disorders. MedlinePlus
Explore Further
Related conditions & procedures
Septoplasty is often part of a broader functional nasal evaluation. These pages explain the related conditions and procedures.
Deviated Septum
The condition septoplasty is designed to correct.
Read moreTurbinate Reduction
Frequently combined with septoplasty when enlarged turbinates also obstruct airflow.
Read moreNasal Valve Collapse
Repair of the nasal sidewall when it contributes to obstruction.
Read moreSeptorhinoplasty
When the septum and the external nasal shape are addressed together.
Read moreSinus Surgery
For patients whose obstruction is compounded by sinus disease.
Read moreRequest a Consultation
Begin with an unhurried clinical evaluation.
Read moreThe Most Important Step
Your expert consultation.
A septoplasty consultation is a careful functional evaluation — examination, often endoscopy, and a discussion of whether structural correction will meaningfully change your breathing.