Double Board Certified · ABOto Otolaryngology
Sinus Surgery NYC — Restoring Natural Drainage and Easier Breathing
Sinus surgery in NYC — including endoscopic sinus surgery (FESS) and balloon sinuplasty — treats chronic sinusitis, nasal polyps, and recurrent sinus infections by restoring the sinuses' natural drainage. For Manhattan patients who have spent years cycling through antibiotics and nasal sprays, Dr. Mourad evaluates your symptoms, CT imaging, and anatomy carefully before any operation is considered.
ABFPRS
Facial Plastic & Reconstructive Surgery
ABOto
Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
In Consultation
"Surgery is the last step, not the first."
A Note from Dr. Mourad
"Most of my sinus patients arrive tired — years of antibiotics, sprays, and infections that never fully clear, and an understandable worry that surgery will be aggressive or will not last. It is not the first answer, and it is not right for everyone. When it is the right answer, the goal is simple: reopen the sinuses' natural drainage, preserve healthy tissue, and let you breathe and sleep again."
— Dr. Moustafa Mourad, MD
Medically reviewed by Moustafa Mourad, MD, FACS — dual board-certified Facial Plastic & Reconstructive Surgeon and Otolaryngologist (Head & Neck Surgery).
Last reviewed: June 2026
Overview
What is sinus surgery?
Sinus surgery is a group of procedures that re-open the natural drainage pathways of the paranasal sinuses — the air-filled spaces behind the cheeks, between the eyes, and in the forehead. The aim is not to remove the sinuses but to restore the airflow and natural mucus clearance that chronic inflammation, polyps, or narrow anatomy has blocked.
Most modern sinus surgery is performed endoscopically — through the nostrils, with no external incisions and no facial bruising — using a small camera and precise instruments to widen the natural openings of the sinuses. In carefully selected patients it can relieve facial pressure, congestion, post-nasal drip, recurrent infections, headaches, and a reduced sense of smell that have persisted despite medication.
Surgery is considered only after chronic sinusitis, recurrent acute sinusitis, nasal polyps, fungal sinusitis, or a structural problem has been documented on examination and CT imaging, and after appropriate medical therapy has been given a fair trial. The right operation is matched to the diagnosis — never the other way around.
The choice between endoscopic sinus surgery and balloon sinuplasty is made from your CT scan and the actual pattern of disease: extensive disease, polyps, or fungal sinusitis usually calls for endoscopic surgery, while focal narrowing may be suited to gentle balloon dilation. Allergy, asthma, and inflammatory management is planned alongside surgery, because controlling the underlying disease protects the long-term result. Dr. Mourad cares for sinus patients across Manhattan — the Upper East Side, Park Avenue, Fifth Avenue, Lenox Hill, Midtown, and near Central Park — as well as Westchester, Long Island, Connecticut, New Jersey, and the wider tri-state area.
Recognizing the Problem
Symptoms of Chronic Sinusitis and Recurrent Sinus Infections
Sinusitis is inflammation of the sinus lining, and its symptoms overlap with colds and allergies — part of why chronic sinus disease so often goes under-treated. The signs below are the most common reasons patients seek evaluation, particularly when they persist beyond ten days, keep returning, or last more than twelve weeks despite treatment.
Facial Pain & Pressure
A heavy, aching pressure across the cheeks, around the eyes, the forehead, or the bridge of the nose — often worse when bending forward.
Nasal Congestion & Obstruction
A persistently blocked or stuffy nose that makes breathing through the nose difficult and can disrupt sleep.
Discharge & Post-Nasal Drip
Thick nasal discharge, or mucus draining down the back of the throat that triggers throat clearing and a lingering cough.
Reduced Smell or Taste
A dulled or absent sense of smell — and, with it, taste — common when inflammation or polyps block the airflow that carries scent.
Headache & Dental Pressure
Headaches and a pressure sensation in the upper teeth, both of which can stem from inflamed sinuses behind the face.
Fatigue, Cough & Ear Fullness
Ongoing tiredness, a lingering cough, ear fullness, and bad breath that can accompany prolonged sinus inflammation.
Acute sinusitis usually settles within a few weeks. Symptoms that last beyond twelve weeks, or that keep returning, point to chronic or recurrent sinusitis and are worth a formal evaluation with nasal endoscopy and, when indicated, CT imaging.
An Established Academic Authority
Double board certification. Fellowship director. Published author. A surgeon's surgeon.
ABFPRS
Board Certified
American Board of Facial Plastic & Reconstructive Surgery
ABOto
Board Certified
American Board of Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
American Academy of Facial Plastic and Reconstructive Surgery
Textbook
Published Author
Contributions to the academic literature of facial plastic surgery
Dual board certification in both Facial Plastic & Reconstructive Surgery and Otolaryngology — Head & Neck Surgery.
02 · Ideal Candidates
Who is a candidate for sinus surgery?
The strongest candidates are patients whose chronic or recurrent sinus symptoms have not resolved despite an appropriate trial of medical therapy, and whose CT imaging and nasal endoscopy show findings that explain those symptoms. Allergy, asthma, and aspirin sensitivity are common alongside sinus disease and are factored into the plan. Candidacy is always confirmed in person — including for children and adolescents, who are evaluated with particular conservatism.
I
Chronic Sinusitis
Facial pressure, congestion, post-nasal drip, and recurrent infections that have persisted for months despite antibiotics, nasal sprays, and saline rinses, with CT findings that match the symptoms.
II
Structural Obstruction & Polyps
A deviated septum, enlarged turbinates, or nasal polyps that physically block the natural sinus openings — often the mechanical reason medication alone has not worked.
III
Recurrent Acute Disease
Frequent, repeated sinus infections through the year that clear with antibiotics but keep returning, disrupting work, sleep, and daily life.
If this describes you, the next step is a quiet, unhurried conversation — not a sales call.
An Honest Note
When sinus surgery may not be right for you.
If appropriate medical therapy has not yet been given a fair trial, that comes first — for many patients, controlling allergy and inflammation resolves symptoms without an operation.
When CT imaging and endoscopy do not show findings that explain the symptoms, surgery is unlikely to help, and the cause is investigated further before any procedure is considered.
Uncontrolled medical conditions, certain bleeding risks, or medications that must remain uninterrupted may make surgery inadvisable until they are addressed and optimized.
Sinus surgery treats sinus and nasal disease; it is not a stand-alone cure for headaches or sleep apnea, which are separate diagnoses evaluated on their own terms.
03 · Approaches
Sinus surgery techniques in NYC.
Modern sinus care is a toolkit. The right approach for a given patient is built from one or several of these techniques, guided by CT imaging and the actual disease pattern.
1 of 6 · Functional Endoscopic Sinus Surgery
04 · Technique
Endoscopic FESS vs balloon sinuplasty.
Two of the most common questions patients ask are whether they need full endoscopic surgery or the gentler balloon procedure, and how the two differ. The honest answer is that it depends on your CT scan and the actual pattern of disease — the two techniques are sometimes even combined in a single operation, using the right tool for each sinus.
FESS
Endoscopic visualization & precise correction
Functional endoscopic sinus surgery uses small rigid endoscopes passed through the nostril to see the sinus openings directly, remove obstructive tissue or polyps, and restore natural drainage — all without external incisions.
It is the right tool when disease is extensive, when polyps are present, when fungal disease is involved, or when the ethmoid cells need structural correction. It is also the workhorse of revision surgery, where prior scarring and altered anatomy demand direct visualization.
Balloon
Gentle dilation, no tissue removal
Balloon sinuplasty uses a soft inflatable catheter to gently widen narrowed sinus openings without removing tissue. Recovery is typically brief, and selected procedures can be performed in the office under local anesthesia.
It is well suited to patients with focal narrowing and limited mucosal disease. It is not a substitute for full endoscopic surgery when polyps, fungal disease, or extensive inflammation are present — choosing it in the wrong patient simply postpones the right operation.
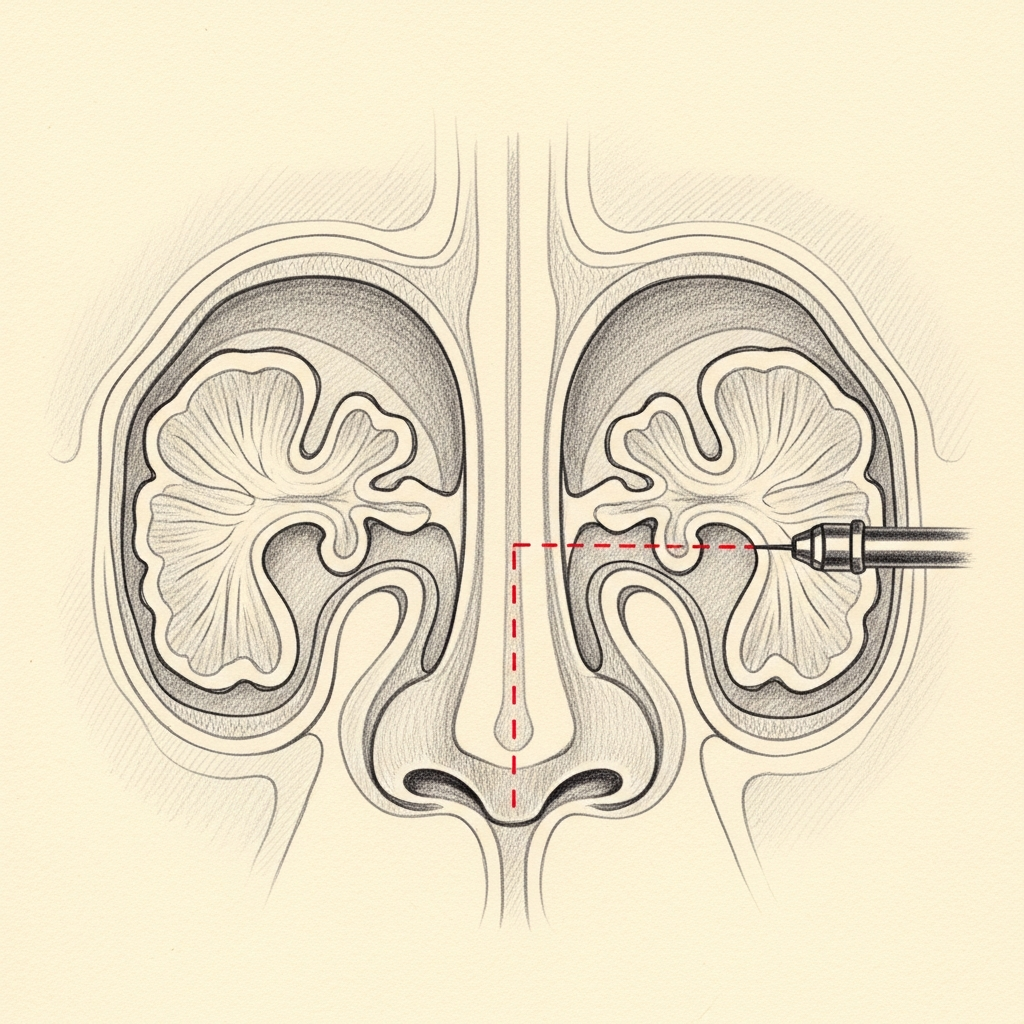
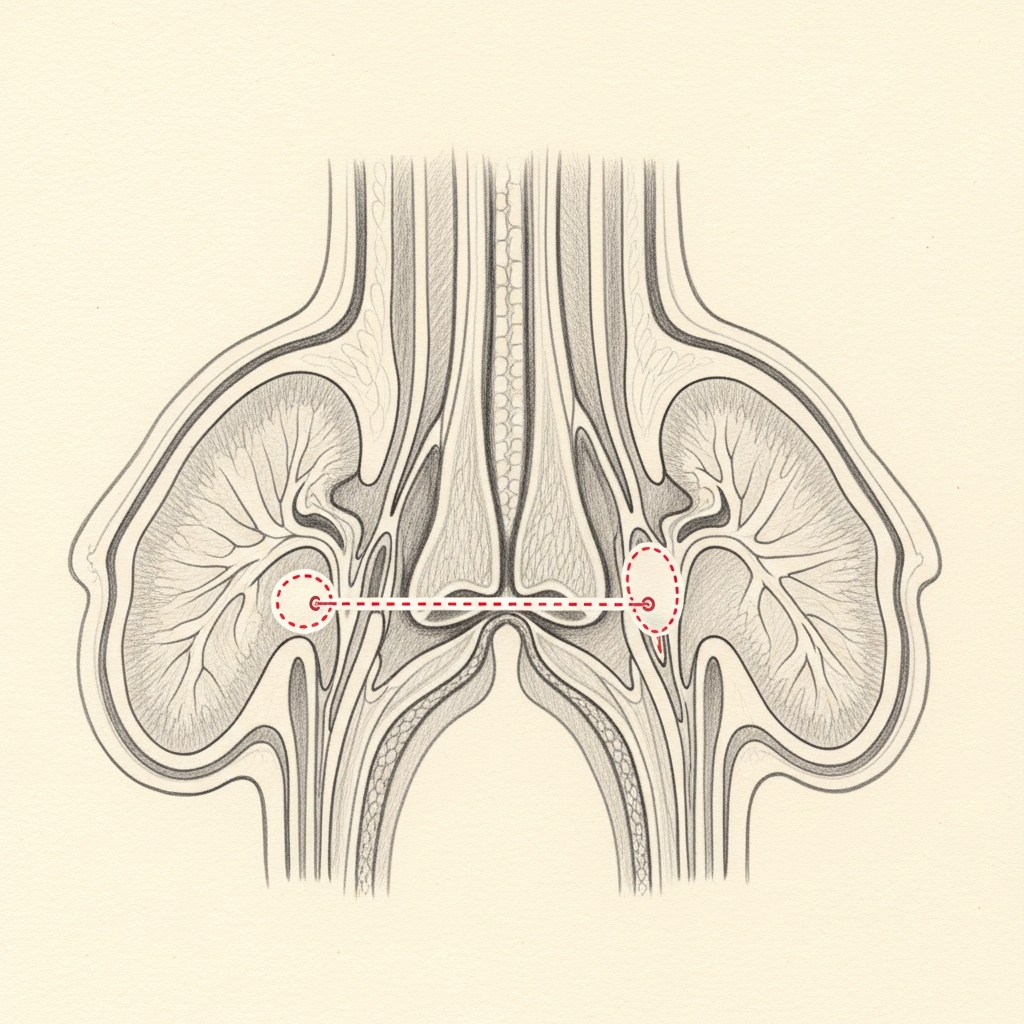
Illustrative diagrams. CT-guided decision-making determines the right combination of techniques for each patient.
01 · Why Dr. Mourad
Why patients choose Dr. Mourad for sinus surgery.
Dr. Mourad is double board-certified in Otolaryngology — Head & Neck Surgery and in Facial Plastic & Reconstructive Surgery. That combination matters for the sinus patient: the same anatomy that governs how you breathe also governs the structure of the nose, so when both are involved they can be evaluated and addressed together within one coordinated plan.
His practice is built around a careful, anatomy-first evaluation. Every plan begins with nasal endoscopy and a review of your CT imaging to understand exactly where drainage is obstructed, so the operation opens precise pathways and preserves healthy tissue rather than removing it broadly.
Complex and revision sinus cases — patients who have had surgery elsewhere that did not fully resolve their symptoms, or who were told their anatomy was difficult — are a routine part of the practice. Patients are referred from across Manhattan and the tri-state area for exactly these situations. Every recommendation is made conservatively, and surgery is offered only when imaging and symptoms genuinely point to it.
Begin the conversation
Discuss your symptoms with Dr. Mourad — a consultation is a clinical evaluation, not a sales conversation.
Cost, Financing & Insurance
How much does sinus surgery cost in NYC?
Sinus surgery cost depends on the diagnosis, imaging findings, extent of sinus disease, and whether treatment involves endoscopic sinus surgery, balloon sinuplasty, turbinate reduction, nasal polyps, image guidance, septoplasty, or combined nasal airway surgery.
Because sinus surgery is a functional, medically documented procedure rather than a cosmetic one, most patients are billed through their medical insurance instead of paying a single flat out-of-pocket fee. The portion a patient ultimately owes depends on their deductible, co-insurance, and plan benefits.
Unlike purely cosmetic procedures, sinus surgery may be covered by insurance when it is medically necessary. Coverage often depends on symptoms, exam findings, CT imaging, prior medical treatment, and the requirements of the patient’s insurance plan. Our office can help review benefits and guide patients through the preauthorization process when appropriate.
What May Affect Cost
- Diagnosis and severity of sinus disease
- CT imaging findings
- Prior medical treatment
- Type of sinus procedure
- Whether septoplasty or turbinate reduction is included
- Insurance plan requirements
This information is educational and is not a guarantee of pricing, insurance coverage, reimbursement, financing approval, or surgical candidacy. A personalized estimate is provided after consultation. Insurance coverage depends on the patient’s plan, medical necessity, documentation, and carrier requirements. Financing terms are determined by third-party financing providers.
05 · In Dr. Mourad's Words
Sinus & airway videos.
Short educational films and patient perspectives from the Manhattan practice.
Dr. Mourad in Practice
An overview of the practice — sinus, airway, and facial plastic surgery in Manhattan.
Patient Perspective
A patient discusses life before, during, and after sinus surgery.
Inside the Consultation
How Dr. Mourad evaluates symptoms, imaging, and surgical candidacy.
Illustrated Anatomy
How sinus surgery opens the drainage pathway.
Sinus procedures are not documented with before-and-after photographs — the relevant anatomy sits behind the face, not on its surface. The illustration shows the natural drainage pathway that endoscopic sinus surgery is designed to restore.
Illustrative anatomy · Not a patient photograph
06 · Recovery
Recovery from sinus surgery.
Stage 01
First 24 Hours
Sinus surgery is almost always an outpatient procedure, so most patients go home the same day with a driver. Light oozing from the nose is expected and is managed with a small gauze drip pad; mild congestion and fatigue are normal. Rest with the head elevated, avoid blowing the nose, and keep activity gentle. Most patients are comfortable with acetaminophen or the medication Dr. Mourad prescribes.
Stage 02
Week 1
The first week is the most noticeable phase of recovery. Congestion, mild pressure, and a stuffy head-cold sensation are common as the lining begins to heal. Saline rinses, started as directed, are the single most important part of aftercare — they keep the newly opened drainage pathways clear of crusting. Many patients return to desk or remote work within a few days, while strenuous exercise and heavy lifting are deferred.
Stage 03
Weeks 2 – 4
Crusting gradually clears and breathing steadily improves. A follow-up endoscopy and gentle in-office debridement help the sinuses heal open rather than scar closed — a routine, well-tolerated part of the process. Most patients resume normal exercise within two to four weeks, once Dr. Mourad confirms healing is on track.
Stage 04
Months 1 – 6
The sinus lining continues to mature over several months. Facial pressure, post-nasal drip, and recurrent infections typically continue to settle as the tissue normalizes. For patients with polyps, allergy, or asthma, ongoing medical therapy — saline rinses, topical steroids, and allergy management — helps protect the result and reduce the chance of recurrence.
Have a specific question?
Send a brief note describing your anatomy or concerns — the office will route it directly to Dr. Mourad for review.
Long-Term Results
Fewer infections, easier breathing, better sleep.
When the natural drainage pathways are restored, many patients experience steady, lasting relief — fewer infections, less facial pressure, clearer breathing through the nose, and for some a gradual return of the sense of smell.
Easier nasal breathing often improves sleep as well: less nighttime congestion and mouth-breathing, and for some patients better tolerance of CPAP therapy. Sinus surgery is not a treatment for obstructive sleep apnea itself, which is evaluated separately, but the airway and the way you sleep are genuinely connected. Individual results vary with the underlying diagnosis.

Insurance & Out-of-Pocket Planning
Insurance and out-of-pocket planning.
Sinus surgery is most commonly billed through medical insurance when chronic disease and structural obstruction are documented. CT imaging and an in-office endoscopy guide the conversation.
Out-of-pocket portions vary by plan. The practice handles pre-authorization in advance so that financial expectations are clear before scheduling.

Before You Arrive
Your consultation, prepared.
Bring any prior CT scans of the sinuses on disc or via portal access.
List your symptom history — when congestion started, what makes it worse.
Bring a complete list of prior medications, antibiotics, and nasal sprays.
Note any allergies, asthma, or aspirin sensitivity.
Allow 60 minutes; expect an in-office nasal endoscopy.
No decisions are made at the first visit — that is by design.
Patient Perspectives
From patients of the practice.
I had chronic sinus pressure for years and had tried every antibiotic. After surgery I can finally breathe through my nose and the headaches are gone. I wish I had done it sooner.
Dr. Mourad explained the CT scan to me carefully and only recommended surgery after we had exhausted medical options. The recovery was easier than I expected.
I came in skeptical because two prior consultations had pushed me toward surgery immediately. Here we tried a course of treatment first, and when that failed, the surgical plan was clearly the right step.
After balloon sinuplasty my recovery was quicker than I expected — I was back at work within a few days, and the saline rinses made a real difference in healing.
I travel in from Westchester and it was worth it. The CT review was thorough, and I am no longer cycling through antibiotics every season.
Individual experiences. Results and recovery vary by patient. Testimonials shared with written consent.
Patient Reviews
Sinus Surgery Patient Experiences
Selected public patient reviews. Individual experiences vary.
“I can now say I can breathe better than I ever have”
Real patient experiences
Selected public reviews from patients of the practice.
Your privacy matters
We never share personal health information.
Board-certified expertise
Dual board-certified facial plastic and reconstructive surgeon.
Individual results vary. Reviews reflect individual experiences and are not a guarantee of outcome.
Questions & Answers
Sinus surgery NYC FAQs
Candidates for surgery are patients with recurrent or chronic sinus symptoms despite appropriate medical therapy, typically including at least 4–12 weeks of topical steroids and a trial of antibiotics when indicated. Surgery is considered when objective findings on nasal endoscopy and CT correlate with persistent symptoms. Medical optimisation—control of allergy, reflux, and smoking cessation—remains an important parallel step. Final candidacy is established after in‑person evaluation and imaging review.
An anatomy‑first assessment prioritizes nasal endoscopy and sinus CT to map drainage pathways, ostia, and zones of obstruction. The review identifies whether disease is driven by structural narrowing (ostial stenosis, concha bullosa, septal deviation) or diffuse mucosal inflammation such as polyposis. Planning focuses on opening precise drainage routes and preserving healthy mucosa to restore normal physiology. This targeted approach guides the choice between dilation, limited tissue removal, or more extensive ethmoid work.
FESS uses endoscopic instruments to remove obstructing tissue and enlarge natural ostia; it is selected when there is diseased mucosa, polyps, or anatomic obstruction requiring tissue removal. Balloon sinuplasty dilates the natural ostia without resecting mucosa and is appropriate for isolated ostial narrowing, especially in the frontal, maxillary, or sphenoid sinuses. Recovery is typically shorter with balloon sinuplasty—often 3–7 days—whereas more extensive FESS usually requires 7–14 days for initial recovery. Choice depends on CT anatomy, mucosal disease burden, and patient goals.
Many patients report reduced frequency of acute infections and less facial pressure within 6–12 weeks as mucosal healing and improved drainage occur. Visualisation at nasal endoscopy and early debridement in the first 1–3 postoperative visits help speed recovery. Some symptom improvement can appear within days to weeks, but maximal functional gains are often evident by 3 months. Ongoing medical therapy for inflammation may still be necessary.
Surgical improvement in smell depends on the underlying cause; patients with obstruction or polyp disease often experience measurable gains after mucosal disease is addressed. When smell loss is due to chronic inflammation without mechanical obstruction, recovery is less predictable and may require continued medical therapy. Early improvement may appear within weeks, but olfactory recovery can continue for 3–12 months. A candid discussion during consultation sets realistic expectations for each case.
Common short‑term issues include bleeding, crusting, and transient nasal congestion; most are managed with routine postoperative care. Less common complications include infection requiring antibiotics, prolonged adhesions, or the need for limited in‑office debridement. Rare but serious risks—such as orbital injury or cerebrospinal fluid leak—are infrequent and mitigated by careful preoperative planning and intraoperative navigation when indicated. All risks are reviewed during the informed consent discussion.
Revision cases are often more complex because normal landmarks may be altered and scarring can obscure drainage pathways; this increases operative time and the need for staged planning. Preoperative CT review is essential to identify prior openings, retained disease, or iatrogenic narrowing. Revision surgery frequently uses intraoperative image guidance and may combine septal or turbinate procedures to optimize access. Outcomes depend on the extent of residual disease and control of underlying inflammation.
High‑resolution CT of the sinuses is the central study, revealing ostial stenosis, mucocele, anatomic variants, and prior operative changes. Nasal endoscopy in clinic documents mucosal condition and nasal airway dynamics. Allergy testing, culture, or systemic evaluation may be recommended when inflammation or fungal/odontogenic causes are suspected. Routine laboratory testing is individualized based on medical history and anesthesia requirements.
When a deviated septum or enlarged turbinates contribute to obstructed airflow, septoplasty or turbinate reduction can be combined with sinus procedures to address both drainage and airway function. Combining these procedures is common and planned when preoperative assessment shows concurrent anatomic obstruction. In some complex cases, staging the interventions improves precision and healing. The specific operative plan is tailored to the patient’s anatomy and symptoms.
Most endoscopic sinus surgeries are performed under general anesthesia in an outpatient surgical facility, although limited balloon dilation can be performed under monitored anesthesia care or local sedation in selected patients. Typical perioperative planning includes preoperative medication review and arrangements for same‑day discharge with an escort. Patients should expect a clinic follow‑up within 3–10 days for initial evaluation and any early debridement; subsequent visits are scheduled based on recovery.
Nasal and sinus obstruction can fragment sleep, increase mouth-breathing, and contribute to snoring. When chronic congestion, a deviated septum, or enlarged turbinates are part of the picture, addressing them can make breathing through the nose at night easier and, for some patients, improve tolerance of CPAP therapy. Sinus surgery is not a stand-alone treatment for obstructive sleep apnea, which is a separate diagnosis requiring a formal sleep evaluation. Dr. Mourad reviews how your nasal and sinus anatomy relates to your sleep and coordinates with a sleep physician when appropriate.
Sinus surgery is frequently billed through medical insurance when chronic or recurrent disease and structural obstruction are documented on examination and CT imaging. Coverage depends on your symptoms, exam and imaging findings, prior medical treatment, and the specific requirements of your plan; purely cosmetic components are not covered. The office reviews your benefits and handles pre-authorization before scheduling, so your out-of-pocket expectations are clear in advance.
Dr. Mourad reviews your medications in advance and will tell you whether to pause blood thinners or certain supplements to reduce bleeding. You may be asked to begin saline rinses or a short course of medication to calm inflammation before the procedure. Arrange for someone to drive you home, and plan a few quiet days for the first phase of recovery. Bring any prior CT scans and a complete symptom and medication history to your pre-operative visit.
By reopening the natural drainage pathways, sinus surgery is intended to provide lasting relief, and many patients have durable improvement in congestion, facial pressure, and recurrent infections. Longevity depends on the underlying disease: patients with allergy, asthma, or nasal polyps have an ongoing inflammatory condition, so continued medical therapy — saline rinses, topical steroids, and allergy management — helps protect the result and reduce the chance of recurrence. Individual results vary, and Dr. Mourad sets realistic expectations for your specific diagnosis.
Clinical references
This page draws on published clinical practice guidelines and public-health references. These sources inform general patient education and do not replace an individual evaluation with Dr. Mourad.
- 01Rosenfeld RM, Piccirillo JF, Chandrasekhar SS, et al. Clinical Practice Guideline (Update): Adult Sinusitis. Otolaryngology–Head and Neck Surgery. 2015;152(2_suppl):S1–S39. AAO-HNSF guideline
- 02U.S. National Library of Medicine (MedlinePlus). Sinusitis. MedlinePlus
- 03Centers for Disease Control and Prevention. Sinus Infection (Sinusitis). CDC
Explore the Sinus Center
Related sinus care & resources
Sinus surgery is one part of a wider program of sinus and airway care. These pages explain the specific techniques, the conditions they treat, and what recovery and cost look like.
Endoscopic sinus surgery (FESS)
The definitive endoscopic operation for chronic rhinosinusitis and obstructive sinus disease.
Read moreBalloon sinuplasty
A tissue-sparing dilation of the sinus outflow tracts for selected patients with focal disease.
Read moreChronic sinusitis treatment
Medical and surgical options for sinus inflammation lasting beyond twelve weeks.
Read moreNasal polyps treatment
How polyps are removed and managed long-term to keep the airway and drainage open.
Read moreRecurrent sinus infections
Why infections keep returning, and when surgery becomes the more durable answer.
Read moreSinus surgery recovery timeline
What healing actually looks like, week by week, after sinus surgery.
Read moreSinus surgery cost & insurance
How sinus surgery is typically billed through insurance and what affects out-of-pocket cost.
Read moreThe Most Important Step
Your expert consultation.
A sinus consultation with Dr. Mourad begins with a detailed history of your symptoms, prior treatments, and what daily life actually looks like for you — the missed work, the disrupted sleep, the seasons spent on antibiotics. He then performs an in-office nasal endoscopy and reviews your CT imaging with you, pointing out exactly where drainage is obstructed. From that, you will leave understanding your diagnosis, the realistic options — including the option not to operate — and what each would involve. No decisions are made under pressure, and patients from across the tri-state area are welcome.