Double Board Certified · Minimally Invasive Sinus Surgery
Balloon Sinuplasty — a gentle approach to chronic sinus disease.
Balloon sinuplasty is not the answer for every sinus problem — but for the right patient with the right pattern of disease, it is one of the most rewarding minimally-invasive procedures in modern rhinology.
ABFPRS
Facial Plastic & Reconstructive Surgery
ABOto
Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
In Consultation
"For the right patient, balloon sinuplasty is a quietly transformative procedure — short downtime, durable relief."
A Note from Dr. Mourad
"Balloon sinuplasty is not the answer for every sinus problem — but for the right patient with the right pattern of disease, it is one of the most rewarding minimally-invasive procedures in modern rhinology."
— Dr. Moustafa Mourad, MD
Medically reviewed by Moustafa Mourad, MD, FACS — dual board-certified Facial Plastic & Reconstructive Surgeon and Otolaryngologist (Head & Neck Surgery).
Last reviewed: June 2026
Is this the right page for you?
This page is for
- You have recurrent acute or limited chronic sinusitis driven by narrowing of the natural sinus drainage openings.
- Your CT scan and examination show focal obstruction without significant polyps or extensive mucosal disease.
- You want a tissue-sparing option that can often be done under local anesthesia with a short recovery.
You may be looking for
- If your disease is extensive or polyp-driven, endoscopic sinus surgery is usually the more appropriate procedure.
- If your main problem is a deviated septum or enlarged turbinates, see septoplasty or turbinate reduction.
Overview
What is balloon sinuplasty?
Balloon sinuplasty is a minimally invasive procedure that opens blocked sinus drainage pathways using a small balloon catheter. The balloon is guided into the natural opening of the sinus, gently inflated to dilate the passage, and removed — preserving the mucosal lining rather than cutting or removing tissue.
It is most useful in patients with recurrent acute sinusitis or limited chronic sinusitis whose disease is driven by anatomic narrowing of the natural sinus openings, in the absence of significant polyps or extensive disease. The right candidate is identified on examination and CT, not by symptom alone.
Balloon sinuplasty can be performed in the office under local anesthesia or in the operating room under general anesthesia, often combined with septoplasty or turbinate reduction when those problems contribute to obstruction. It is not a substitute for traditional endoscopic sinus surgery when the disease is extensive.
An Established Academic Authority
Double board certification. Fellowship director. Published author. A surgeon's surgeon.
ABFPRS
Board Certified
American Board of Facial Plastic & Reconstructive Surgery
ABOto
Board Certified
American Board of Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
American Academy of Facial Plastic and Reconstructive Surgery
Textbook
Published Author
Contributions to the academic literature of facial plastic surgery
Dual board certification in both Facial Plastic & Reconstructive Surgery and Otolaryngology — Head & Neck Surgery.
02 · Ideal Candidates
Who benefits most from this operation.
Candidacy is determined together at consultation. The most satisfied patients share three things in common.
I
Documented Chronic Sinusitis
Recurrent sinus infections or persistent sinus symptoms with imaging evidence of mucosal disease at the sinus outflow tracts.
II
Failed Medical Therapy
Symptoms that persist despite adequate trials of antibiotics, topical steroids, and saline irrigation.
III
Favourable Anatomy
Sinus anatomy on imaging that is suited to balloon dilation — typically maxillary, frontal, and sphenoid outflow tracts.
If this describes you, the next step is a quiet, unhurried conversation — not a sales call.
An Honest Note
When this operation may not be right for you.
Significant nasal polyposis is generally better treated with formal endoscopic sinus surgery, not balloon alone.
Severe anatomic variations or extensive disease beyond the outflow tracts require traditional FESS.
Active dental or odontogenic sources of sinus disease are addressed first.
Allergic disease is medically optimised before any surgical intervention.
03 · Approaches
The full range of options.
Balloon sinuplasty is a setting decision as much as a technique decision. The right plan considers where it is performed, whether full endoscopic surgery would be more appropriate, and which companion procedures should travel with it.
1 of 6 · In-Office Balloon
04 · Technique
Balloon vs endoscopic surgery.
The two operations are complementary, not competitive. Balloon dilation is gentle and tissue-sparing; formal endoscopic surgery is more comprehensive when needed.
Balloon
Tissue-Sparing
A small flexible balloon is positioned within the sinus outflow tract and gently inflated to dilate the natural opening. No tissue is removed.
Recovery is brief, the natural mucosa is preserved, and the procedure can often be performed under local anesthesia in the appropriate patient.
FESS
Endoscopic Tissue Surgery
Formal endoscopic sinus surgery uses precision instruments to remove diseased tissue and open the sinuses widely. It is the right operation for more extensive disease.
FESS and balloon are often combined within a single procedure — balloon for selected sinuses, formal surgery for those that require it.
Illustrative diagrams. The right balance is determined individually based on imaging and disease pattern.
01 · Why Dr. Mourad
A surgeon trusted by surgeons for this operation.
Dr. Moustafa Mourad is double board-certified by the American Board of Facial Plastic & Reconstructive Surgery and the American Board of Otolaryngology — Head & Neck Surgery, and serves as an AAFPRS Fellowship Director.
The practice concentrates on the operations of the face, nose, and sinuses — and on the patients other surgeons have found challenging.
Every consultation is unhurried, every plan is individual, and no operation is recommended unless it is the right one.
Begin the conversation
Chronic sinus symptoms? An honest evaluation of whether balloon, FESS, or medical therapy is the right next step.
Cost, Financing & Insurance
Balloon Sinuplasty Cost, Financing & Insurance in NYC
Balloon sinuplasty cost depends on which sinuses are treated, the extent of sinus disease, whether the procedure is performed in office or in an operating room, and whether it is combined with other nasal or sinus treatment.
As a treatment for chronic sinus symptoms, balloon sinuplasty may be covered by insurance when it is medically necessary. Coverage often depends on symptoms, CT imaging, prior medical treatment, and the requirements of the patient’s insurance plan. Our office can help review benefits and guide patients through preauthorization when appropriate.
What May Affect Cost
- Number of sinuses treated
- Severity of sinus disease
- In-office vs operating room setting
- CT imaging findings
- Prior medical treatment
- Insurance plan requirements
This information is educational and is not a guarantee of pricing, insurance coverage, reimbursement, financing approval, or surgical candidacy. A personalized estimate is provided after consultation. Insurance coverage depends on the patient’s plan, medical necessity, documentation, and carrier requirements. Financing terms are determined by third-party financing providers.
05 · In Dr. Mourad's Words
Educational videos.
Short educational films and patient perspectives from the Manhattan practice.
Dr. Mourad in Practice
An overview of the practice and philosophy.
Patient Perspective
A patient discusses her experience before, during, and after surgery.
Inside the Consultation
How Dr. Mourad evaluates anatomy, goals, and candidacy.
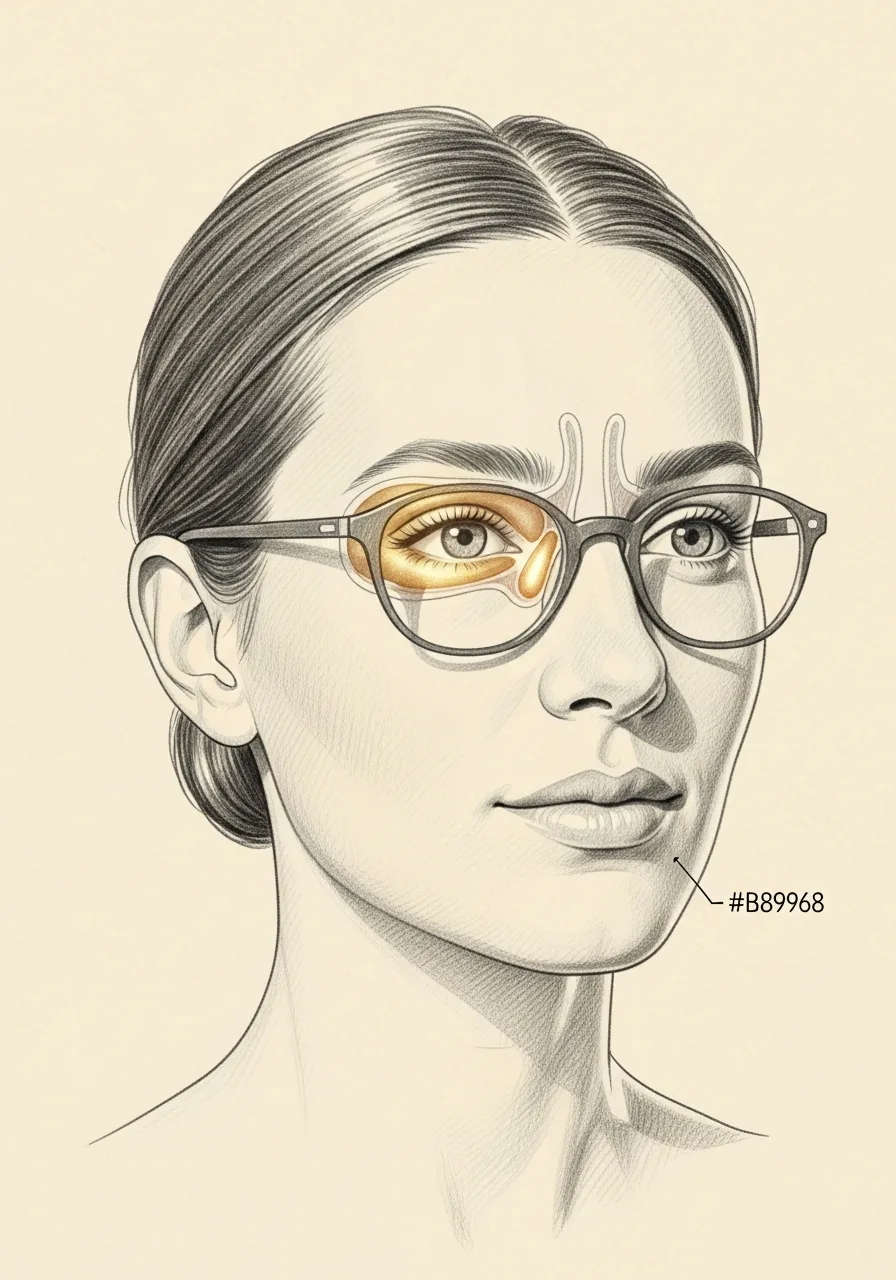
Illustrated Anatomy
How balloon sinuplasty restores drainage.
Balloon sinuplasty is performed on internal anatomy that does not photograph from the outside. The illustration shows how a small balloon gently dilates the natural sinus ostium without removing tissue.
Illustrative anatomy · Not a patient photograph
06 · Recovery
What healing actually looks like.
Stage 01
First 24 Hours
Most patients return home within an hour of an in-office procedure. Mild congestion and discomfort are typical for the first day.
Stage 02
Week 1
Through the first week, saline irrigation supports healing. Most patients return to office work the day after the procedure.
Stage 03
Weeks 2 – 4
Through weeks two to four, the dilated outflow tracts continue to settle and drainage steadily improves. Most patients notice meaningful symptom relief.
Stage 04
Months 1 – 12
Long-term, the durability of relief depends on the underlying disease — many patients experience years of symptom improvement.
Have a specific question?
Send a brief note describing your anatomy or concerns — the office will route it directly to Dr. Mourad for review.

Before You Arrive
Your consultation, prepared.
Bring any prior sinus CT scans for review.
List the antibiotics, steroids, and irrigations you have tried, and for how long.
Note any allergies, asthma, or aspirin-sensitivity.
List current medications, including blood thinners and supplements.
Allow 45 minutes for a focused sinus evaluation, often including endoscopy.
Bring questions about in-office versus operating-room options.
Patient Perspectives
From patients of the practice.
I was back at work the next morning. The pressure in my forehead that I had carried for years was simply gone within a few days.
Dr. Mourad made it very clear when balloon was the right answer and when it was not. I appreciated that he did not oversell it.
After two rounds of antibiotics each winter, I was ready for something more durable. The procedure itself was much easier than I had imagined.
Individual experiences. Results and recovery vary by patient. Testimonials shared with written consent.
Frequently Asked
Patient questions, honestly answered.
Balloon sinuplasty is a catheter-based ostial dilation technique performed under endoscopic visualization. The device rides over a guidewire to the sinus ostium and the balloon is inflated to enlarge the natural opening. The intent is to re-establish ventilation and mucociliary clearance with minimal mucosal removal. Final candidacy and the exact technical plan require CT review and an in-person exam.
Traditional endoscopic sinus surgery often requires targeted tissue removal to open sinus corridors. Balloon sinuplasty focuses on widening the ostium without routine resection of mucosa or bone, following a tissue-preserving philosophy. The two approaches can be complementary and are chosen based on anatomy and disease pattern. Your surgeon will explain when dilation alone is reasonable versus when adjunctive instruments are necessary.
Candidacy depends on multiplanar CT findings, symptom history, and response to medical therapy. Favorable CT features include focal ostial narrowing with otherwise preserved sinus anatomy and little or no polyp burden. Candidates will have typically completed topical steroids and irrigations before procedural consideration. Definitive candidacy is determined during consultation with CT review and endoscopic assessment.
Selected patients may undergo office-based dilation with topical anesthesia and local infiltration. Office procedures require appropriate patient selection for anxiety, comorbidity, and nasal anatomy, and they include monitoring and preprocedure counseling. Many procedures are completed in 30–90 minutes depending on how many sinuses are treated. If combined procedures are planned, the operating room under general anesthesia may be more appropriate.
Common immediate effects include nasal congestion, mild bleeding, and facial pressure for several days. Less frequent complications include infection, persistent symptoms, or rarely adjacent structure injury; these are discussed during informed consent. Many patients return to desk work in 48–72 hours and to moderate activity within 1–2 weeks, though recovery varies by individual and combined procedures. Close postoperative surveillance with saline irrigations and clinic review is standard.
Duration of symptom improvement varies with underlying inflammatory disease and adherence to postoperative therapy. Some patients note relief within weeks, while others require ongoing topical treatment to maintain benefit. Chronic drivers such as allergy or polyposis affect long-term durability and are managed alongside surgical care. Recurrence of symptoms prompts endoscopic reassessment and repeat imaging to guide further management.
Revision cases demand careful review of prior operative reports and current CT anatomy because scarring and altered landmarks change the approach. Balloon dilation can be considered in select revisions where ostial narrowing persists without extensive scar or polyp load. In many revision scenarios, targeted scar release or tissue removal is also required. Detailed preoperative planning and intraoperative flexibility are essential for safe, effective revision work.
Balloon dilation is not the primary treatment for significant nasal polyps or invasive fungal disease. Those conditions usually require targeted removal, debridement, and disease-specific medical therapy. Dilation may be an adjunct in mixed disease when ostial patency contributes to symptoms, but decisions are individualized after CT and endoscopic assessment. Patients with polyps typically expect a combined surgical and medical strategy.
Common concurrent procedures include septoplasty, turbinate reduction, and nasal valve repair when indicated by exam and CT. Combining work addresses multi-level obstruction and can improve overall symptom control. The need for additional procedures is determined at consultation and may shift the case to the operating room. Each combined plan is tailored to the patient’s anatomy and goals.
Dr. Mourad begins with a focused history, endoscopic nasal exam, and multiplanar CT review to assess ostial architecture and prior surgical change. He discusses prior medical therapy, comorbidities such as allergy or AERD, and realistic goals for symptom control. The plan emphasizes tissue preservation when appropriate and explains when adjunctive tissue removal or revision strategies are required. Final decisions are made in person with shared decision-making.
Clinical references
This page draws on published clinical practice guidelines and public-health references. These sources inform general patient education and do not replace an individual evaluation with Dr. Mourad.
- 01Rosenfeld RM, Piccirillo JF, Chandrasekhar SS, et al. Clinical Practice Guideline (Update): Adult Sinusitis. Otolaryngology–Head and Neck Surgery. 2015;152(2_suppl):S1–S39. AAO-HNSF guideline
- 02U.S. National Library of Medicine (MedlinePlus). Sinusitis. MedlinePlus
- 03Centers for Disease Control and Prevention. Sinus Infection (Sinusitis). CDC
Explore the Sinus Center
Related sinus care & resources
Balloon sinuplasty is one approach among several. These pages compare it to full endoscopic surgery, explain the conditions it treats, and describe recovery and cost.
Sinus surgery in NYC
The overview of every sinus technique and how the right operation is matched to the diagnosis.
Read moreEndoscopic sinus surgery (FESS)
The more comprehensive operation for extensive disease, polyps, or fungal sinusitis.
Read moreChronic sinusitis treatment
Medical and surgical options for sinus inflammation lasting beyond twelve weeks.
Read moreBalloon sinuplasty vs sinus surgery
An honest comparison of when each operation is the right choice.
Read moreWhat to expect after balloon sinuplasty
A practical recovery guide for the days and weeks after the procedure.
Read moreSinus surgery cost & insurance
How sinus procedures are typically billed and what affects out-of-pocket cost.
Read moreThe Most Important Step
Your expert consultation.
A balloon sinuplasty consultation is a careful sinus evaluation — examination, often endoscopy, and review of imaging to determine whether balloon, formal surgery, or further medical therapy is the right next step.