Double Board Certified · AAFPRS Fellowship Director
Preservation Rhinoplasty in NYC — refine the silhouette, keep the anatomy.
Dr. Moustafa Mourad (ABFPRS, ABOto) offers an anatomy-first preservation rhinoplasty approach in NYC. Learn when push-down or let-down may be appropriate.
ABFPRS
Facial Plastic & Reconstructive Surgery
ABOto
Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director

In Consultation
"Preservation suits the right candidate — the examination decides."
A Note from Dr. Mourad
"Preservation rhinoplasty is not a marketing term — it is a different philosophy of nasal surgery. Instead of reducing and reconstructing, we lower the dorsum as one intact unit and keep the natural dorsal aesthetic line that the patient was born with."
— Dr. Moustafa Mourad, MD
Key takeaways
- Preservation rhinoplasty lowers the bridge as one unit instead of removing and rebuilding it.
- The dorsal aesthetic lines you were born with — the natural bridge contour — are kept intact.
- It suits selected primary patients with a smooth dorsal hump and good tip support.
- It is one tool among several, not a replacement for structural rhinoplasty.
- Septal correction for breathing can be combined in the same operation when needed.
Overview
What is preservation rhinoplasty?
Preservation rhinoplasty is a modern approach to nasal surgery that preserves the dorsal aesthetic lines of the nose rather than disassembling and rebuilding them. Instead of removing the hump and reconstructing the bridge, the underlying skeleton is lowered as a single unit so the surface anatomy of the dorsum is left intact.
For appropriately selected primary rhinoplasty patients — typically those with a smooth dorsal hump and good tip support — preservation technique can produce a natural-looking bridge with less disruption to the soft-tissue envelope. It is one tool among several, not a replacement for structural rhinoplasty.
Preservation is not the right answer for every nose. Significant tip refinement, marked asymmetry, prior surgery, very thick or very thin skin, and complex deformities are often better addressed with a structural approach. The decision is made in consultation, after a careful examination of the bony, cartilaginous, and soft-tissue anatomy.
Planning & Cost
Preservation Rhinoplasty Cost
Preservation rhinoplasty is priced within the primary rhinoplasty framework, but final cost depends on the patient's anatomy, whether a push-down, let-down, hybrid, or structural approach is appropriate, the extent of tip and septal work, functional airway treatment, operative time, anesthesia, and facility requirements.
Learn more about primary rhinoplasty cost in NYC.
An Established Academic Authority
Double board certification. Fellowship director. Published author. A surgeon's surgeon.
ABFPRS
Board Certified
American Board of Facial Plastic & Reconstructive Surgery
ABOto
Board Certified
American Board of Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
American Academy of Facial Plastic and Reconstructive Surgery
Textbook
Published Author
Contributions to the academic literature of facial plastic surgery
Dual board certification in both Facial Plastic & Reconstructive Surgery and Otolaryngology — Head & Neck Surgery.
02 · Ideal Candidates
Who benefits most from preservation.
Preservation rhinoplasty rewards careful selection. The four profiles below describe the anatomy and goals that tend to suit the technique; the only way to know whether your nose qualifies is a physical and, where helpful, endoscopic examination.
I
Smooth, Modest Dorsal Hump
A small to moderate dorsal hump with otherwise good dorsal aesthetic lines is the most consistent indication. When the bridge contour is essentially favorable and only needs lowering, the dorsum can often be settled as one unit rather than reduced and rebuilt.
II
Strong Native Support & Favorable Skin
Intact tip support and skin that is neither very thick nor very thin help the underlying change translate cleanly to the surface. Primary noses without prior surgery or significant trauma are generally better suited than scarred or previously operated noses.
III
Subtle, Identity-Preserving Goals
Patients who want a refined nose that still looks like their own — a quieter change to the profile rather than a transformed nose — align well with the philosophy of keeping the dorsal lines they were born with.
IV
Functional Planning When Needed
When a deviated septum or airway concern is also present, septal correction can be planned in the same operation. Preservation of the dorsum and functional work on the septum are combinable when the anatomy allows.
If this describes you, the next step is a quiet, unhurried conversation — not a sales call.
An Honest Note
When preservation rhinoplasty may not be right for you.
Preservation is not the right answer for every nose. Marked asymmetry, a deviated bony pyramid, or an irregular dorsum frequently needs the control of a structural approach to produce straight, balanced lines.
Significant tip refinement, very thick or very thin skin, and complex deformities are often better served by removing and rebuilding the framework rather than preserving it.
Revision surgery — operating on a nose that has already been altered — usually involves scar tissue and changed anatomy that favor a structural plan, sometimes with cartilage grafting.
If examination shows preservation is not appropriate, Dr. Mourad will say so directly and explain the structural alternative rather than force the technique to fit.
03 · Approaches
Six variations of preservation.
Preservation is not a single technique — it is a family of approaches. The right variation depends on the height of the hump, the strength of the tip, and the goals of the patient.
1 of 6 · Dorsal Preservation
04 · Technique
Dorsal preservation vs traditional reduction.
The two strategies differ in how the bridge is changed. Preservation lowers the existing dorsum as one unit; traditional reduction takes the hump down from above and rebuilds the lines. Neither is universally better — the anatomy decides.
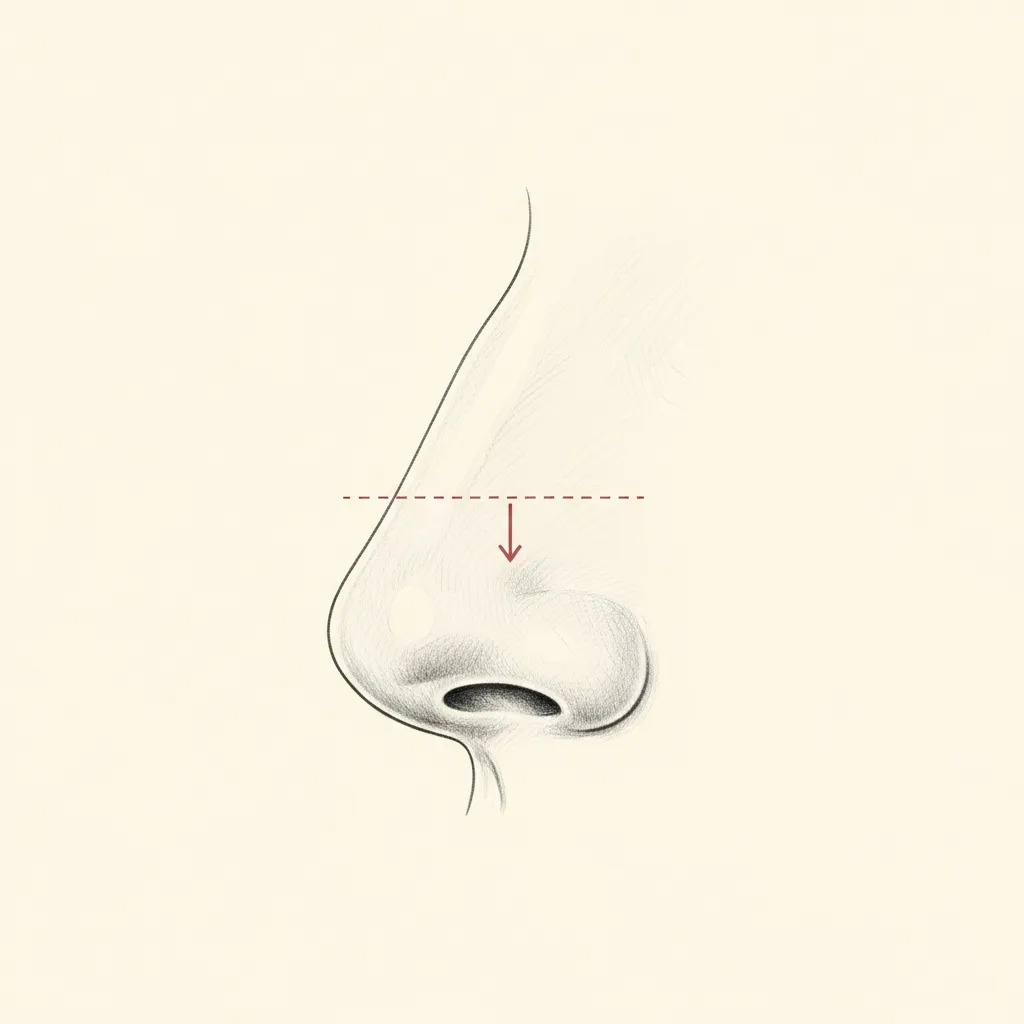
Preservation
Push-down — dorsum stays intact
Dorsal preservation lowers the dorsum by removing a strip of bone and septum at the base of the nasal pyramid, allowing the entire dorsal segment to settle downward as a single intact unit.
The natural dorsal aesthetic lines, the keystone area, and the cartilaginous dorsum are preserved — which is why the result can look less operated for the right candidate.
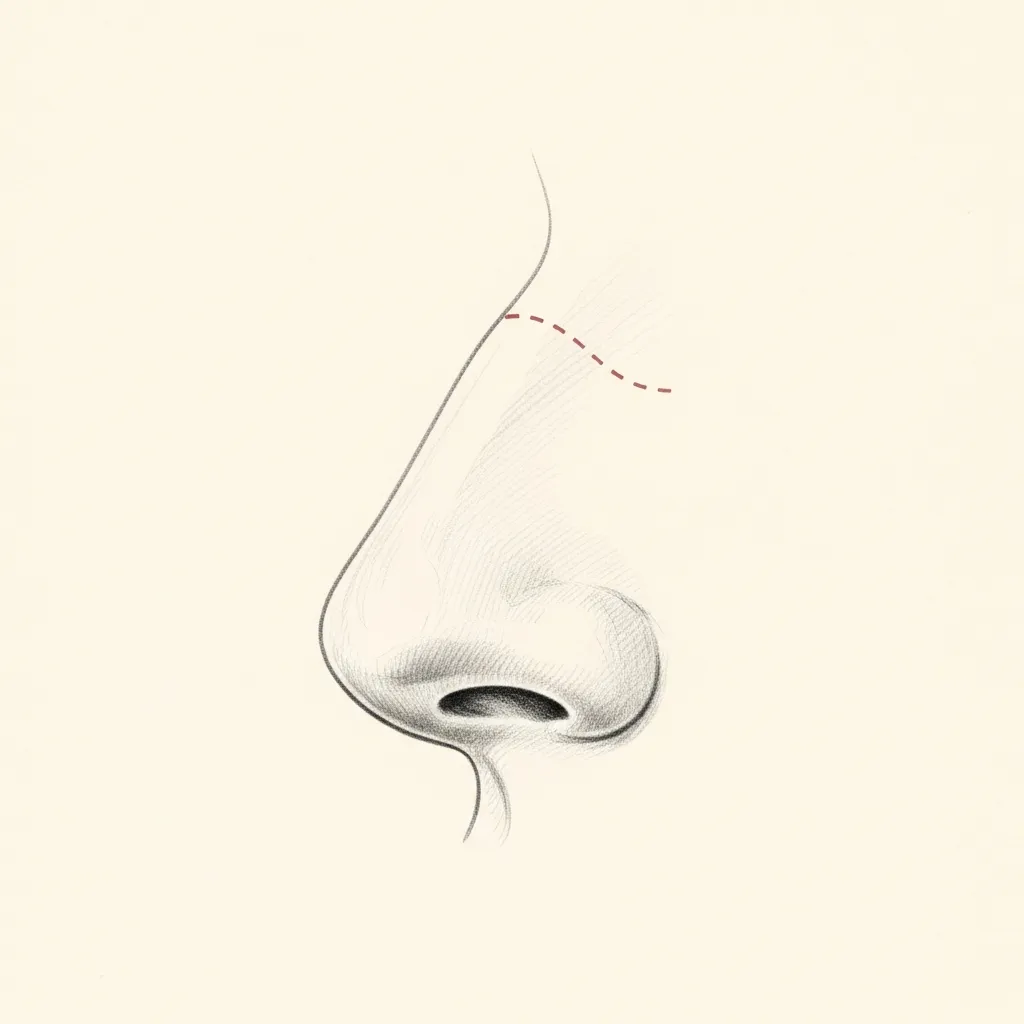
Traditional
Component reduction & reconstruction
Traditional reduction approaches the hump from above, rasping or cutting the bony and cartilaginous dorsum directly. Reconstruction of the dorsal lines — often with spreader grafts — is then required.
Traditional techniques offer greater versatility in cases that require significant reshaping or revision of prior surgery. Both approaches can produce strong results in the right hands.
Illustrative diagrams. Technique selection is individualized based on dorsal anatomy, skin character, and surgical goals.
05 · At a Glance
Three approaches, side by side.
A simplified comparison of how the surgical strategies differ. It is an educational overview, not a substitute for examination — most plans are individualized and some combine elements of more than one approach.
| Traditional Dorsal Reduction | Dorsal Preservation | Hybrid Structural-Preservation | |
|---|---|---|---|
| Tissue handling | Hump removed from above; bone and cartilage reduced directly. | Dorsum lowered as one intact unit by removing bone and septum at the base. | Dorsum preserved where possible; selected structural work added where needed. |
| Dorsal aesthetic lines | Reconstructed after reduction, often with spreader grafts. | Native lines preserved. | Native lines preserved over the dorsum; refined structurally elsewhere. |
| Internal valve support | May require grafting to maintain or restore valve support. | Keystone area left intact, which can help maintain valve anatomy. | Valve addressed directly when structural support is required. |
| Typical candidate | Larger or irregular humps, asymmetry, revision, major reshaping. | Primary noses with a smooth hump and good support. | A preservable dorsum alongside a tip or area needing structural refinement. |
| Recovery character | Swelling and timeline vary with the extent of reshaping. | Swelling and timeline vary by individual; the soft-tissue envelope is less disrupted. | Reflects the combined scope of preservation and structural elements. |
| Main limitations | More dissection of the dorsal lines that then need rebuilding. | Not suited to marked asymmetry, thick/thin skin extremes, or revision. | Planning is more complex; depends on which areas are preserved. |
| When chosen | When the dorsum needs significant reshaping or correction of prior work. | When the existing dorsal lines are favorable and only need lowering. | When part of the nose suits preservation and part needs structure. |
Comparison is general and educational. The appropriate approach for any individual is determined in consultation after examination.
01 · Why Dr. Mourad
Modern preservation, classically trained.
Dr. Moustafa Mourad approaches preservation rhinoplasty as an anatomy-driven decision. His preoperative evaluation includes a focused history, high-resolution photography in multiple views, and both external and endoscopic nasal examination. He documents dorsal convexity, radix position (the nasal root), tip support, septal alignment, and turbinate size. When prior surgery exists, he reviews operative records and imaging. These data determine whether push-down or let-down is feasible and whether concurrent functional procedures are required.
Quantitative mapping guides intraoperative choices. Dr. Mourad measures the hump's peak relative to the radix, assesses the osseocartilaginous transition, and palpates the bony pyramid for asymmetry. He evaluates skin thickness and soft-tissue mobility to predict how underlying change will translate to the surface. If the internal nasal valve or septum poses functional risks, he plans septoplasty (septum correction) or valve stabilization as part of the operation. This layered planning reduces the chance of unexpected intraoperative conversion and supports airway preservation.
Dr. Mourad's dual board certification in facial plastic surgery and otolaryngology informs a balanced aesthetic and functional perspective. He explains the tradeoffs between preservation and structural strategies and describes clear contingency plans should tissue behavior require grafting or conversion to a structural approach.
Begin the conversation
A consultation is a clinical evaluation — not a sales conversation.
In Dr. Mourad's Words
Preservation rhinoplasty videos.
Short educational films and patient perspectives from the Manhattan practice.
Rhinoplasty with Dr. Mourad
An overview of Dr. Mourad's approach to rhinoplasty in his Manhattan practice.
Patient Perspective
A patient discusses her experience before, during, and after surgery.
Inside the Consultation
How Dr. Mourad evaluates anatomy, goals, and surgical candidacy.
From the Patient Gallery
Rhinoplasty Before and After Cases
A selection of documented rhinoplasty results from the Manhattan practice, photographed in standardized studio conditions with written photographic consent on file. These are general rhinoplasty cases shown to illustrate Dr. Mourad's aesthetic — they are not all preservation-technique cases. Individual results vary with anatomy and goals; these cases are representative, not predictive.

Primary Rhinoplasty · Female, 20s
Primary rhinoplasty addressing dorsal contour and tip refinement, with the goal of preserving the patient's natural facial proportions. The comparison views show pre-operative and post-operative anatomy at the five standard clinical photography angles.

Primary Rhinoplasty · Female, 30s

Primary Rhinoplasty + Sinus Surgery · Female, 40s

Primary Rhinoplasty · Female, 20s
Pre and post-operative comparison · Photographed in standardized studio conditions · Written consent on file
06 · Recovery
What healing actually looks like.
Stage 01
First 24 – 72 Hours
Expect a cast or splint on the bridge, mild to moderate swelling, and bruising that is often most noticeable around the eyes. Rest with the head elevated and use cold compresses as directed. Some oozing from the nostrils is normal in the first day or two. Contact the office for the red-flag signs listed below rather than waiting.
Stage 02
Week 1
The external cast typically comes off around the end of the first week. The bridge will still be swollen and the result will not yet represent the final shape. Most people feel ready to return to desk work and quiet daily activity around this time, though this varies by individual.
Stage 03
Weeks 2 – 4
Bruising fades and the most visible swelling continues to settle. Light activity is gradually resumed on Dr. Mourad's guidance; strenuous exercise, contact sports, and anything that risks a blow to the nose are still avoided. Glasses may need to be supported off the bridge as advised.
Stage 04
Months 1 – 3
The nose looks progressively more natural as deeper swelling resolves. Many patients feel comfortable in social and professional settings during this window, while subtle refinement of the tip and bridge continues beneath the surface.
Stage 05
Months 6 – 12+
Residual swelling — especially at the tip — resolves slowly, and dorsal lines continue to mature over many months. Final shape is best judged across this longer horizon rather than in the early weeks. Timelines are individual and depend on anatomy and the extent of work performed.
When to call the office
- Fever, increasing redness, or warmth around the nose
- Bleeding that does not slow with gentle pressure and head elevation
- Sudden, worsening, or one-sided pain not controlled by prescribed measures
- Pus-like discharge or a foul smell
- Shortness of breath, chest pain, or calf swelling — seek emergency care
A Common Question
Does preservation mean less swelling or faster recovery?
Because preservation lowers the dorsum as one unit and disturbs the soft-tissue envelope less than removing and rebuilding the bridge, some patients do experience a relatively settled early recovery. That is a reasonable expectation for the right candidate — but it is not a guarantee, and it is not true of every nose.
Recovery depends far more on individual anatomy, skin character, whether functional work was performed, and how each person heals than on the label of the technique. Swelling — particularly at the tip — resolves slowly with any rhinoplasty, and the final shape matures over many months regardless of approach.
The honest answer is that preservation is chosen for the quality and naturalness of the result it can give the right candidate, not as a shortcut to a faster recovery. Dr. Mourad will give you a realistic timeline for your specific plan at consultation.
Have a specific question?
Send a brief note describing your anatomy or concerns — the office will route it directly to Dr. Mourad for review.
Six Months to a Year
Long-term results.
Over six months to a year, deeper swelling resolves and the dorsal lines settle into their mature contour. Because the native dorsum is preserved rather than rebuilt, the bridge tends to read as a quieter, more natural version of the nose the patient began with.
Long-term stability still depends on individual anatomy and healing. Dr. Mourad follows patients across this longer horizon and discusses what to expect — and what cannot be promised — before surgery rather than after.

Form & Function
Breathing addressed in the same operation.
When a deviated septum or airway concern accompanies the cosmetic goal, septal correction can be planned in the same setting as the preservation dorsal work, sparing a second operation and a second recovery.
Functional and aesthetic targets are coordinated from the outset. The septum is the foundation the preserved dorsum sits on, so combined planning is approached carefully and individualized to the anatomy.
Further Reading
Preservation rhinoplasty vs structural rhinoplasty
Preservation and structural rhinoplasty are two philosophies rather than competitors. Preservation lowers and reshapes the existing framework as a unit; structural rhinoplasty removes and rebuilds it, often with cartilage grafts. The right choice depends on the anatomy in front of us — dorsal shape, tip support, skin character, and any prior surgery.
Preservation suits many primary noses with a smooth dorsal hump and good support, while a structural approach remains the better answer for marked asymmetry, very thick or very thin skin, revision work, or major reshaping. For a fuller discussion of the thinking behind the technique, read Dr. Mourad's explanation of the preservation rhinoplasty philosophy and how preservation compares to structural rhinoplasty.

Before You Arrive
Your consultation, prepared.
Bring photographs of your nose from earlier in life if you have them.
Note any breathing difficulty — when it began, when it is worst.
List any prior nasal surgery, trauma, or related procedures.
Bring questions. Consultations are designed for a real conversation.
Allow 60 minutes; expect a thorough physical examination.
No decisions are made at the first visit — that is by design.
Frequently Asked
Patient questions, honestly answered.
Preservation rhinoplasty mobilizes and repositions the native osseocartilaginous roof instead of directly excising the dorsal hump. Traditional reduction removes bone and cartilage and then reconstructs the dorsum. Preservation aims to maintain keystone continuity and the native mucosal lining when anatomy permits. It is a selective strategy, not a universal alternative, and the operative plan is individualized at consultation.
Candidacy depends on dorsal convexity shape and position, septal length and alignment, skin thickness, and any prior surgery or trauma. Noses with a single, smooth dorsal convexity and sufficient septal support are more likely to be amenable. Irregular humps, marked dorsal deviation, or prior destabilizing procedures may favor traditional or structural approaches. A hands‑on exam and review of prior operative records determine the final recommendation.
Choice is driven by how much vertical lowering is needed and the relationship of the dorsum to the piriform aperture and maxillary platform. Push‑down translates the dorsal unit inferiorly for modest reductions without creating step‑offs. Let‑down removes a controlled wedge at the lower nasal base when greater lowering is required. Intraoperative assessment of mobility and keystone integrity often finalizes the decision.
Yes. Preservation approaches are commonly combined with septoplasty and targeted valve procedures when airway obstruction exists. Maintaining dorsal continuity does not prevent correction of septal deviation or turbinate hypertrophy. Airway function is assessed and prioritized during preoperative planning, and additional procedures are performed as indicated to protect or improve breathing.
Both closed and open exposures are used, depending on tip work, prior surgery, and grafting needs. Many preservation dorsal maneuvers can be performed through closed intranasal incisions. When precise tip suturing or graft placement is required, a small external transcolumellar incision may be used. Incision choice is based on surgical goals and is discussed during the consent visit.
Most patients have the greatest swelling and discomfort in the first 48–72 hours. Many return to desk work within 7–14 days as visible bruising and early edema improve. Substantial contour softening occurs by 4–8 weeks, but subtle swelling and remodeling continue for 3–12 months. Activity restrictions and follow‑up visits are tailored to the procedure and discussed preoperatively.
Revision and post‑traumatic cases present scar tissue and altered anatomy that may limit preservation options. In select revisions where the dorsal unit and lining remain mobilizable, preservation can be attempted with contingency plans for reconstruction. Many revisions require grafting or staged procedures to restore support and predictability. A careful review of prior records and imaging is essential before planning surgery.
Risks overlap with other rhinoplasty techniques and include contour irregularity, asymmetry, prolonged swelling, septal hematoma, and airway changes. Early complications such as hematoma or acute breathing difficulty are managed promptly and may require surgical intervention. Minor contour concerns can sometimes be addressed with secondary procedures after healing. A frank discussion of risks and mitigation strategies occurs during consent.
Clinical references
This page draws on published clinical practice guidelines and public-health references. These sources inform general patient education and do not replace an individual evaluation with Dr. Mourad.
- 01American Society of Plastic Surgeons. Rhinoplasty — procedure overview and patient information. ASPS
- 02American Academy of Facial Plastic and Reconstructive Surgery — professional society for facial plastic surgeons. AAFPRS
- 03Saban Y, et al. Overview of Dorsal Preservation Rhinoplasty. Facial Plast Surg Clin North Am. 2023. PubMed
- 04Long-Term Follow-Up with Dorsal Preservation Rhinoplasty. Facial Plast Surg Clin North Am. 2023. PubMed
- 05Preservation Rhinoplasty Versus Structural Rhinoplasty in Dorsal Hump Reduction: A Systematic Review and Meta-Analysis of Randomized Controlled Studies. Facial Plast Surg Aesthet Med. 2025. PubMed
Explore Further
Related procedures & resources
Preservation rhinoplasty is one technique among several. These pages explain how it compares to other nasal approaches.
Rhinoplasty NYC
The overview of rhinoplasty approaches offered in the practice.
Read morePrimary Rhinoplasty
Planning a first-time rhinoplasty.
Read moreRevision Rhinoplasty
Correction after a prior nasal operation.
Read moreSeptorhinoplasty
Combined cosmetic and functional correction of the nose and septum.
Read moreBefore & After Gallery
Representative rhinoplasty cases, photographed with written consent on file.
Read moreRequest a Consultation
Begin with an unhurried clinical evaluation.
Read moreThe Most Important Step
Your expert consultation.
A preservation rhinoplasty consultation begins with a comprehensive assessment of your nasal anatomy and a discussion of your aesthetic goals. Dr. Mourad will examine whether your dorsum is preservable and explain candidly whether preservation or a structural approach better fits your nose.