Double Board Certified · Functional Nasal Care
Nasal Turbinate Hypertrophy in NYC — a treatable cause of nasal obstruction.
Learn how enlarged nasal turbinates can cause chronic congestion, nasal obstruction, mouth breathing, and sleep disruption. Evaluation and treatment in NYC with Dr. Mourad.
ABFPRS
Facial Plastic & Reconstructive Surgery
ABOto
Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
In Consultation
"The turbinates do important work — humidifying and filtering. The goal of treatment is to reduce them just enough to restore breathing, never to remove what is needed."
A Note from Dr. Mourad
"Turbinate hypertrophy is a common, treatable cause of chronic nasal obstruction. The right treatment ranges from optimised medical therapy to a focused in-office reduction to operating-room turbinate surgery — matched to severity and patient."
— Dr. Moustafa Mourad, MD
Overview
What is turbinate hypertrophy?
Turbinate hypertrophy is enlargement of the inferior turbinates — the long, scroll-shaped structures along the sidewalls of the nasal passages that warm, humidify, and filter inhaled air. When they swell beyond their normal range, they narrow the airway and obstruct breathing.
The enlargement may be soft-tissue (mucosal) swelling driven by allergic rhinitis, non-allergic rhinitis, or chronic irritation, or it may involve the bony scaffolding of the turbinate itself. It is also frequently a compensatory response to a deviated septum, where the turbinate on the wider side grows to fill the extra space.
Symptoms include chronic nasal obstruction, mouth-breathing, snoring, and disturbed sleep. Diagnosis is made on examination, supplemented by nasal endoscopy. Treatment is layered — medical first, then office or operating-room reduction when medical therapy has not been enough.
Key takeaways
- Turbinate hypertrophy is enlargement of the inferior turbinates that narrows the airway.
- The turbinates warm, humidify, and filter air, so reduction stays conservative.
- Enlargement may be soft-tissue swelling or involve the turbinate's bony framework.
- It often accompanies a deviated septum and may be treated together.
- Treatment is layered — medical first, then office or operating-room reduction.
An Established Academic Authority
Double board certification. Fellowship director. Published author. A surgeon's surgeon.
ABFPRS
Board Certified
American Board of Facial Plastic & Reconstructive Surgery
ABOto
Board Certified
American Board of Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
American Academy of Facial Plastic and Reconstructive Surgery
Textbook
Published Author
Contributions to the academic literature of facial plastic surgery
Dual board certification in both Facial Plastic & Reconstructive Surgery and Otolaryngology — Head & Neck Surgery.
Castle Connolly Top Doctor — Plastic Surgery, 202602 · Symptoms
How this condition typically presents.
Three patterns are most common. Patients often recognise themselves in one or more of these.
I
Persistent Congestion
Chronic nasal obstruction that may switch sides over the course of the day, often worse when lying down.
II
Mouth Breathing & Snoring
Mouth breathing on waking, dry mouth, and snoring — often misattributed to other causes.
III
Postnasal Drip & Sinus Pressure
Persistent postnasal drainage and facial pressure that does not respond fully to standard medical management.
03 · Anatomy
Normal vs hypertrophied turbinate.
The inferior turbinate is a functional structure. The goal of treatment is to bring it back toward normal — never to remove it.
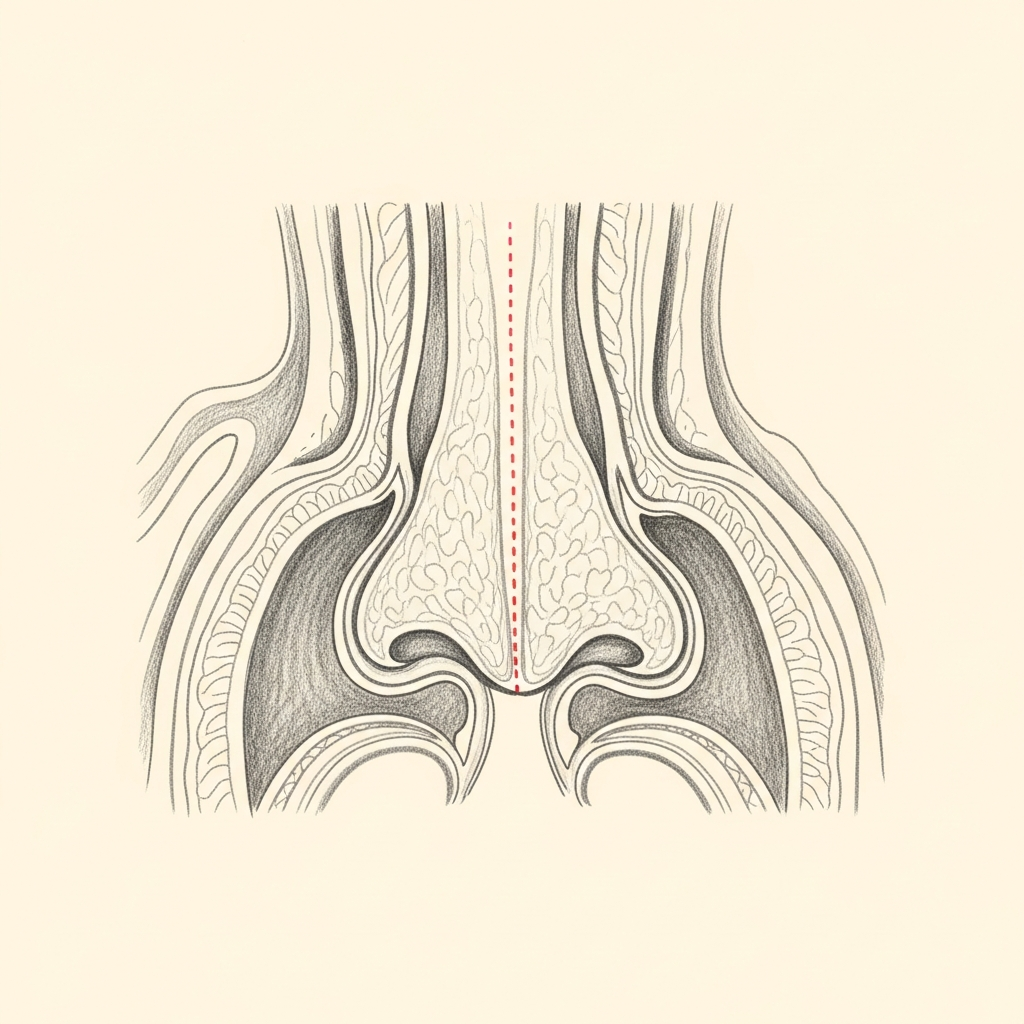
Normal
Functional and appropriately sized
A normal inferior turbinate provides about 50% of the nasal airway resistance that the body uses to humidify, warm, and filter inspired air. It is functional tissue.
When sized appropriately, the turbinate leaves enough airspace between itself and the septum for comfortable nasal breathing.
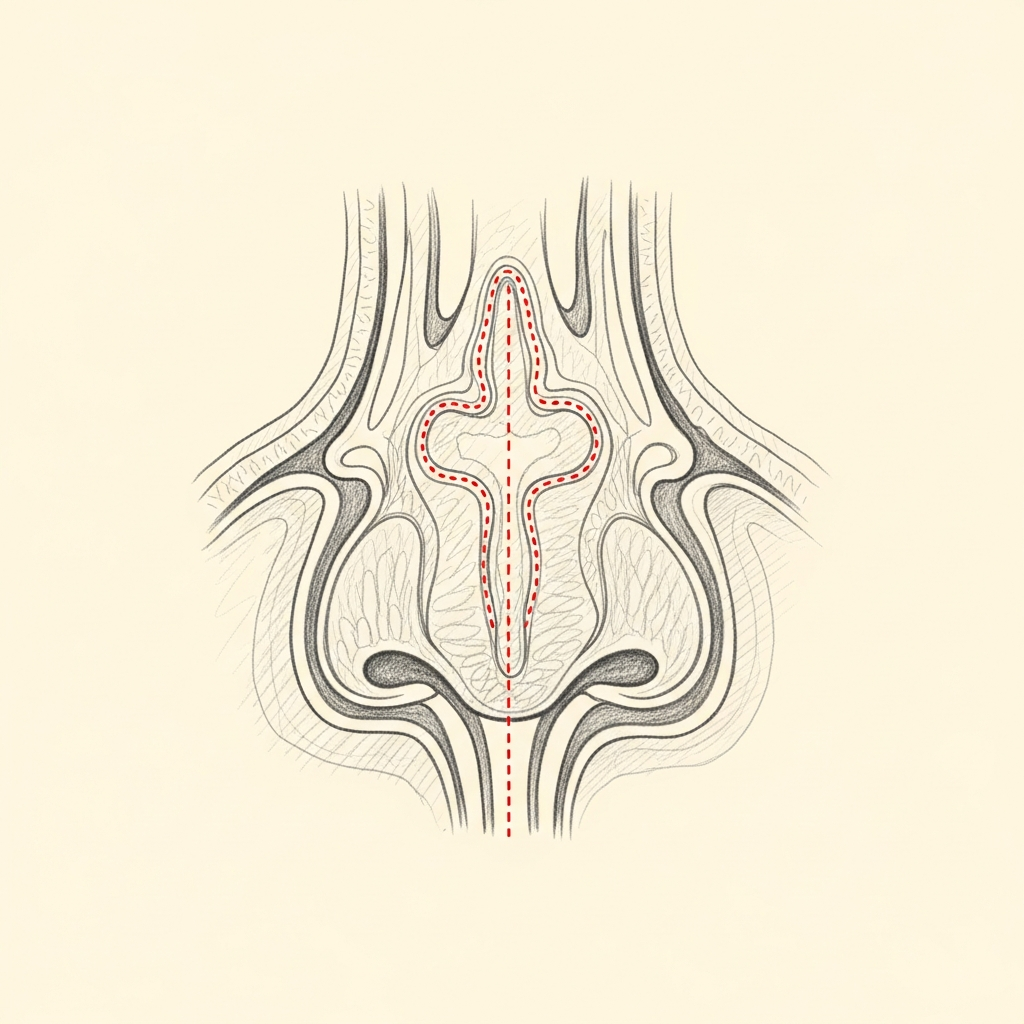
Hypertrophied
Enlarged, obstructive
Hypertrophied turbinates are enlarged most often from chronic allergic or non-allergic inflammation. The submucosal tissue is bulky and obstructive.
Conservative submucosal reduction — preserving the surface mucosa and the bony framework — restores airway without sacrificing the turbinate's essential function.
Illustrative diagrams. Aggressive turbinate resection is avoided as a matter of principle.
04 · Diagnosis
How the diagnosis is made.
Diagnosis is made by anterior rhinoscopy and confirmed with nasal endoscopy.
Allergy testing is recommended when the clinical pattern suggests an allergic component.
CT imaging is reserved for cases where coexisting sinus disease is suspected.
05 · Treatment Options
Treatments matched to the diagnosis.
Treatment is individual. The right answer ranges from optimised medical therapy to a focused procedure to definitive surgery.
Optimised Medical Therapy
Intranasal steroids, antihistamines, and treatment of allergic triggers.
Learn More
Turbinate Reduction Surgery
Conservative submucosal reduction — preserving the function of the turbinate.
Learn More
Combined Septoplasty + Turbinate
Often performed together when both structural deviation and turbinate hypertrophy contribute.
Learn More
01 · Why Dr. Mourad
Diagnosis first, treatment second.
Dr. Mourad evaluates the turbinates as one part of a complete functional examination — turbinate hypertrophy frequently coexists with septal deviation, and the two are often best treated together.
Conservative reduction is the principle: enough to restore airway, never aggressive enough to risk empty-nose-syndrome-type complications.
Medical therapy is optimised before surgical reduction is considered.
When to Seek Care
When to seek care promptly.
Severe facial pain, high fever, or visual changes — evaluate urgently.
New unilateral nasal obstruction in an adult — evaluate within days.
Bloody nasal discharge that does not resolve — evaluate within days.
Significant breathing difficulty disrupting sleep or exertion — schedule evaluation promptly.
Outlook
What to expect.
When the diagnosis is correct and the right treatment is applied, the outlook is generally good. Most patients describe meaningful improvement in symptoms and day-to-day function.
When symptoms persist despite treatment, the workup is re-opened. Persistent symptoms with no answer almost always mean the diagnosis is incomplete.

Living Well
Day-to-day measures that help.
Daily saline irrigation, control of indoor allergens, and good sleep hygiene meaningfully reduce day-to-day symptoms for many patients.
Medical therapy, when prescribed, works best when used consistently rather than as needed — this is one of the most common reasons treatment seems to fail.
Frequently Asked
Patient questions, honestly answered.
Turbinates are layered structures of bone and mucosa on the lateral nasal wall that warm, humidify, and direct airflow. The inferior turbinates most directly alter nasal airway caliber, while the middle turbinates are important for sinus drainage and endoscopic orientation. When turbinates enlarge, nasal resistance increases and breathing effort can change. A focused exam assesses how turbinate anatomy and mucosal state affect a patient’s symptoms.
Temporary congestion usually follows a viral illness, allergen exposure, or short‑term medication use and clears with time or brief treatment. Turbinate hypertrophy denotes sustained tissue bulk that is predominantly mucosal (inflammatory) or structural (submucosal tissue or bone). Inflammatory swelling tends to respond to optimized medical therapy, while structural enlargement may persist despite medication. Differentiation requires history, nasal endoscopy, and selective testing during an office evaluation.
Persistent enlargement arises from chronic inflammatory conditions (allergic or non‑allergic rhinitis), long‑term medication effects, repeated infections, or inherent bony and submucosal bulk. Compensatory enlargement can also occur opposite a deviated septum. Prior nasal surgery changes mucosal architecture and can alter both symptoms and treatment options. Identifying the dominant driver is central to selecting medical versus surgical management.
Evaluation typically begins with a targeted history about symptom triggers, prior therapies, and prior nasal surgery. A physical exam includes anterior rhinoscopy and office endoscopic inspection to assess turbinate size, mucosal appearance, septal alignment, and nasal valve function. Allergy testing or imaging is reserved for cases where inflammation, sinus disease, or structural concerns influence management. Definitive treatment planning requires this in‑person assessment.
Medical therapy is first‑line when mucosal inflammation predominates and includes intranasal anti‑inflammatory measures, saline irrigation, and trigger control. Surgery is considered after an adequate trial of optimized medical care fails, when structural bulk persists, or when combined anatomic problems need correction. The decision balances objective findings, symptom burden, and patient goals and is made during a shared in‑person discussion. Some patients benefit from combined procedures when multiple contributors to obstruction coexist.
Surgeons use mucosal‑sparing approaches such as submucosal resection, radiofrequency ablation, coblation, and limited outfracture to reduce bulk while preserving surface mucosa. Submucosal resection removes submucosal tissue, radiofrequency and coblation apply controlled thermal injury to shrink tissue, and outfracture repositions the turbinate bone. The unifying goal is improved airway caliber with preservation of humidification and mucociliary function. Technique choice depends on the anatomic pattern, prior surgery, and intraoperative findings.
Yes. Turbinate reduction is commonly paired with septoplasty when a deviated septum causes compensatory turbinate enlargement. It may also be part of a functional septorhinoplasty when airway and external shape are both addressed. Combining procedures can correct multiple causes of obstruction in a single operation and streamline recovery. Prior surgery or altered anatomy can complicate planning and often requires tailored mucosal‑preserving strategies.
Early recovery often includes nasal congestion, mild facial pressure, crusting, and occasional light bleeding; saline irrigations and topical care reduce crusts and support healing. Many patients return to sedentary work within 1–2 weeks, with progressive improvement over 3 months as mucosa remodels. Exercise and heavy lifting are typically resumed gradually per the surgeon’s guidance. Follow‑up visits permit debridement if needed and monitor for complications.
Risks include bleeding, infection, persistent congestion, crusting, and, rarely, over‑resection syndromes leading to excessive dryness or empty‑nose symptoms. Preserving mucosa reduces the likelihood of problematic dryness but does not eliminate risk. Recurrence can occur if underlying inflammation persists or compensatory tissue develops; management ranges from renewed medical therapy to targeted revision procedures. Any decision about revision is made after reassessment and after inflammation is controlled.
The Most Important Step
Get an expert evaluation.
A careful evaluation by a double board-certified physician is the right first step. The conversation is unhurried, the diagnosis is honest, and treatment is matched to what you actually have.